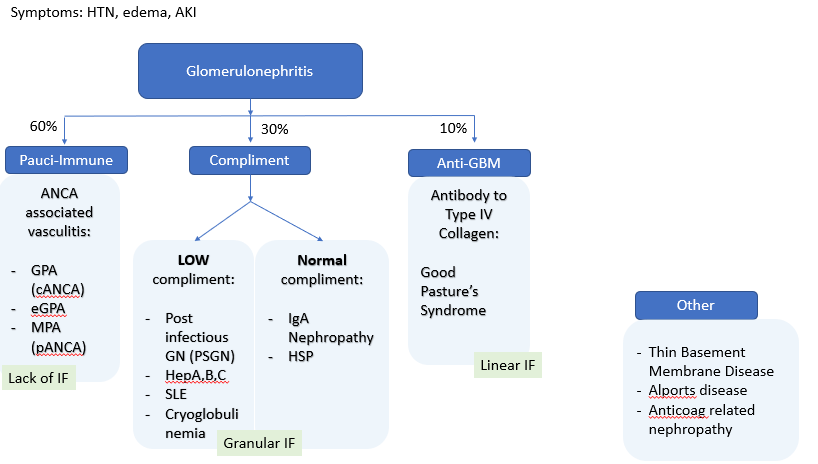
We present a middle aged female iwth chronic TPN use via central line after roun-en-y procedure complicated by necrosis and short gut syndrome who presents with subacute malaise. She is found to have Enterococcus faecium and coagulase negative staph bacteremia. She develops an AKI with UA showing hematuria and proteinuria. Urine sediment shows dysmorphic RBC and muddy brown cast. We reviewed the ddx for glomerulonephritis. Due to elevated ANA and normal ANCA, and low compliment levels, patient was diagnosed with post-infectious GN. She had ASO+ titers.
Post infectious GN is uncommon in >40yo. It is usually due to group A strep however can happen with non-strep bacteria, viruses, parasites, fungi and bacterial endocarditis or VP shunt infection. The source of E. Faecium was thought to be due to a line infection and perhaps endocarditis (although TEE was too high risk to confirm diagnosis). Patient received diuresis and had strong recovery.