
Today we discussed a case about an older woman who presented after subacute painless jaundice and chronic weight loss + fatigue + nausea, found to have new onset DM, mixed cholestatic and hepatocellular liver injury, and a large pancreatic head mass. She was diagnosed with pancreatic adenocarcinoma.
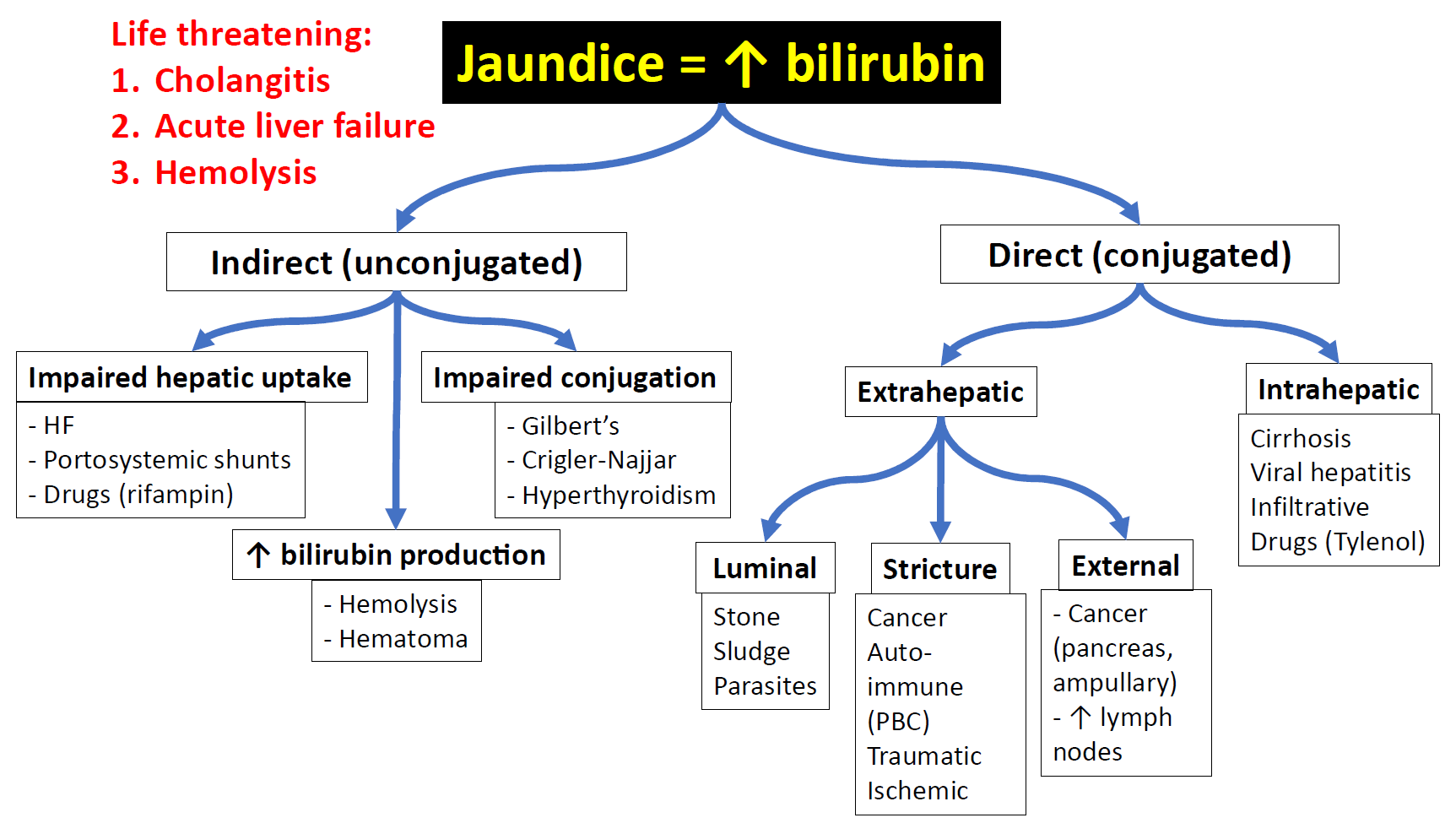
JAUNDICE FRAMEWORK
LIVER INJURY
- The R factor (or R value) could be useful in helping distinguish cholestatic vs hepatocellular liver injury.

PANCREATIC ADENOCARCINOMA
- Definitely be concerned in patients presenting with painless jaundice. But patients with pancreatic cancer can also present with abdominal pain.
- Of the patient diagnosed with pancreatic cancer, up to 2/3 can develop new onset DM in the 36 months surrounding the diagnosis of pancreatic cancer.
- Your illness script should include risk factors such as
- Age > 50
- Hx chronic pancreatitis
- Obesity
- T2DM
- High red meat consumption
- EtOH use disorder
- Tobacco use disorder
- Mucinous cystic lesions of the pancreas
- Inherited conditions (e.g. Peutz-Jeghers syndrome, BRCA2 germline mutations, hereditary pancreatitis, Lynch syndrome)
- CA 19-9 is the most sensitive (70-92%) and specific (68-92%) tumor marker with clinical utility.
- Serial monitoring of CA 19-9 levels can be useful in following patients after potentially curative surgeries and for those receiving chemotherapy for advanced disease.
Rising CA 19-9 levels usually precede the radiographic appearance of recurrent disease.
RESOURCES
