
We discussed a case of an immunocompetent middle-aged man with HTN, HLD, history of diverticulitis, who presented with subacute diarrhea, LLQ to diffuse abdominal pain, nausea + vomiting, decreased PO intake, found to have diverticulitis and CMV colitis.
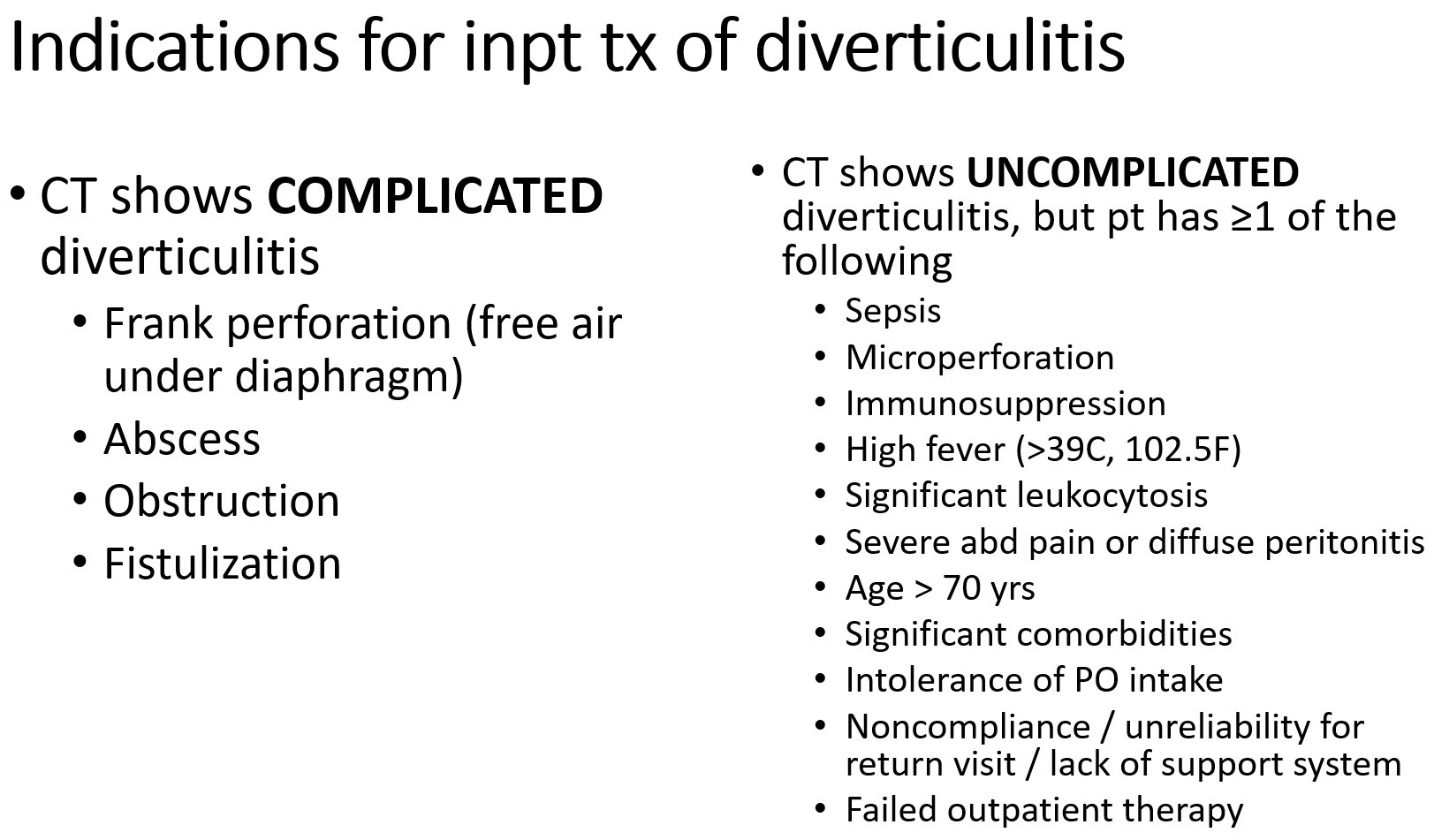
When should a patient be admitted and treated for diverticulitis?
Risk factors for diverticulitis
- A diet low in fiber, high in fat, and high in red meat
- Physical inactivity
- Obesity
- Other medical problems eg Ehler-Danlos, Marfan’s, Williams-Beuren syndromes, HIV, patients undergoing chemotherapy
- Current smokers
One topic that is brought up when talking about risk factors for diverticulitis is seeds and nuts in one’s diet. These are not associated with an increase in risk of diverticulosis, diverticulitis, or diverticular bleeding.
Workup
- Acute diverticulitis is often a clinical diagnosis and does not require imaging to confirm the diagnosis.
- CT Abd/Pelv W Con can help differentiate uncomplicated vs complicated diverticulitis.
- Endoscopic evaluation has no role in establishing the diagnosis of acute diverticulitis. In fact, endoscopy should be avoided in the acute setting due to risk of perforation or exacerbation of existing inflammation.
Highlights in the Management of diverticulitis
- Outpatient treatment includes antibiotics that cover GI organisms (GNR and anaerobes). Some common antibiotics regimen include: ciprofloxacin + metronidazole, augmentin, levofloxacin + metronidazole.
We should expect improvement in symptoms within a few days. Patients should follow-up during this time (in 2-3 days) to ensure symptoms are not progressing, which may warrant inpatient management. - There is some controversy regarding the use of antibiotics in acute uncomplicated diverticulitis. Recommendations from European experts / guidelines tend to be against management with antibiotics, while American experts / guidelines tend to favor the use of antibiotics.
Current evidence suggests antibiotics do not shorten the clinical course of diverticulitis, though some sources suggest antibiotics may help prevent complications (e.g. abscesses) and future episodes of diverticulitis. - Colon cancer can manifest similarly to acute diverticulitis (colicky abdominal pain, LLQ pain, fevers, relief with flatus or BMs).
Therefore, especially in patients who have not undergone recent (w/in 3 years) screening colonoscopies, colonoscopy should be done after resolution of acute diverticulitis (4-8 weeks after) to exclude colon malignancy.
CMV colitis
- Rare in immunocompetent.
In immunosuppressed patients, CMV infection tends to be reactivation of latent disease.
While in immunocompetent patients, CMV infection can also be due to primary infection. - In an immunocompetent patient, serologic testing may help with diagnosis of primary infection either with detection of…
- CMV-specific IgM or
- 4x rise in CMV-specific IgG
- Treatment consists of antiviral therapy e.g. ganciclovir and valganciclovir
References
- Uptodate: Colonic diverticulosis and diverticular disease: epidemiology, risk factors, pathogenesis
- Uptodate: Clinical manifestations and diagnosis of acute diverticulitis in adults
- Uptodate: Acute colonic diverticulitis: medical management
- Uptodate: Epidemiology, clinical manifestations, and treatment of cytomegalovirus infection in immunocompetent adults
- Uptodate: Approach to the diagnosis of cytomegalovirus infection
- Annals of IM: Diverticulitis: myth vs evidence
- NEJM: Diverticulitis
- NEJM case records of the Mass Gen Hospital: Case 8-2020: an 89-year-old man with recurrent abdominal pain and bloody stools
- Cytomegalovirus colitis
- MKSAP 18 GI & Hepatology questions 39 & 74
