
We discussed a case of a younger man with HIV, who presented with subacute fevers, B symptoms, fatigue, progressively worsening SOB with dry cough, found to have diffuse bilateral GGO on CT chest and diagnosed with AIDS and hypoxemic respiratory failure due to Pneumocystis pneumonia.
We reviewed the CD4 count thresholds for antibiotic prophylaxis against a few significant opportunistic infections (OI) in patients with HIV:
One recent update to antibiotic prophylaxis guidelines is for MAC. Primary prophylaxis against MAC is NOT recommended for patients with HIV who immediately initiate ART. Otherwise, for people not on effective ART, the CD4 cutoff to prophylax against MAC is <50 . Read more about this guideline here!

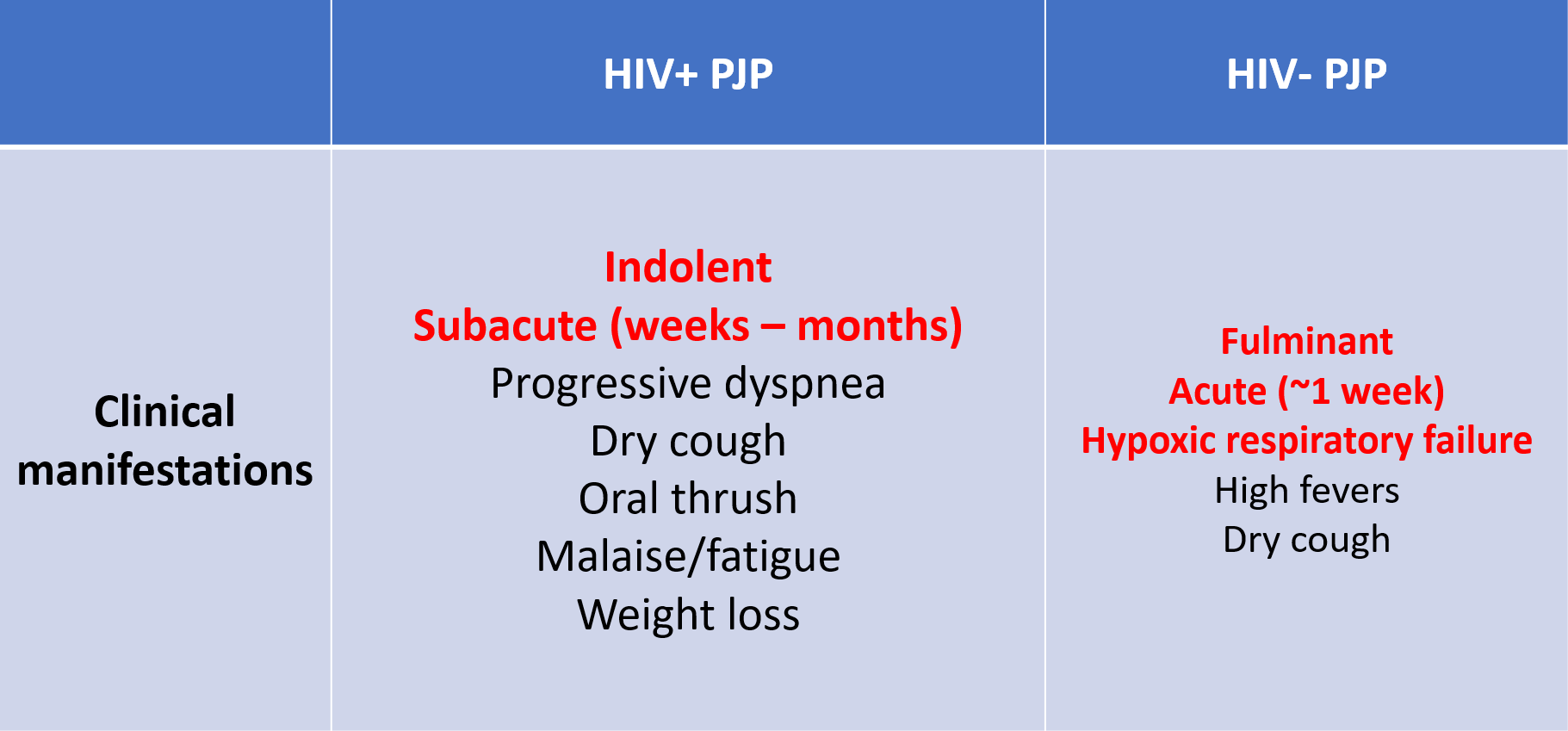
We also discussed the different clinical manifestations between HIV+ PJP pulmonary infection and HIV- PJP pulmonary infection:
Severity of PJP pulmonary infection is dependent on degree of hypoxia:
- Mild
- A-a gradient <35
- PaO2 > 70 mmHg
- Moderate
- A-a gradient 35-45
- PaO2 > 70 mmHg
- Severe
- A-a gradient >45
- PaO2 50-70 mmHg
Besides TMP-SMX for treatment, adjunctive glucocorticoids should be used is specific situations:
- Moderate to severe PJP infection
References:
- Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV
- NEJM: PJP
- Uptodate: Clinical presentation and diagnosis of Pneumocystis pulmonary infection in patients with HIV
- Uptodate: Treatment and prevention of Pneumocystis infection in patients with HIV
- Uptodate: Epidemiology, clinical manifestations, and diagnosis of Pneumocystis pneumonia in HIV-uninfected patients
- Uptodate: Treatment and prevention of Pneumocystis pneumonia in patients without HIV
- IBCC: PJP
