Most common etiologies for BLOODY pleural effusion
-Trauma
-Malignancy
-Pulmonary infarction
-Post-cardiac injury
Differential for Lymphocytic Exudative pleural effusion
–TUBERCULOSIS
-Malignancy (Lung> BRCA, lymphoma, ovarian/gastric)
-Sarcoid
-Rheumatoid pleurisy
-Chylothorax
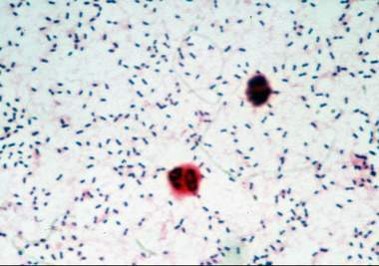
Workup of Suspected Pleural Tb
-Exudative lymphocytic pleural effusion, <10 % eosinophils
-High LDH (usually >500)
-AFB stain and culture (only positive 20-30 % of the time)
-Adenosine deaminase- HIGH sensitivity (if <40) and HIGH specificity (if >60), however depends on laboratory validity
-Pleural biopsy (positive 60-90 %)- can be done either via thoracoscopy or percutaneous needle biopsy)
Treatment
-Airborne isolation (~50 % of patients with concomitant Pulmonary Tb)
-RIPE therapy (similar to pulmonary Tb)

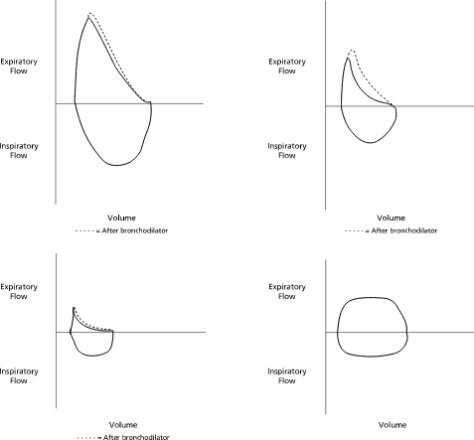 Top Right: Normal; Top Right: Asthma, Bottom Left: COPD, Bottom Right: Fixed Obstruction / Tracheal Stenosis
Top Right: Normal; Top Right: Asthma, Bottom Left: COPD, Bottom Right: Fixed Obstruction / Tracheal Stenosis