
- Autosomal Dominant Polycystic Kidney Disease
- Type 1: ~85%, average age of developing ESRD is around 50yo
- Type 2: ~15%, average age of developing ESRD is around 70yo
- Cardiovascular disease is the most common cause of death in ADPKD and ADPKD is the most common inherited kidney disease
- For an infected renal cyst, use a lipophilic antibiotic (for good cyst penetration) such as quinolones or bactrim
- ADPKD is present in 5-10% of dialysis patients in the US
- Renal manifestations include recurrent UTIs, cyst infection, hematuria from cyst hemorrhage, and nephrolithiasis (usually uric acid stones)
- Extra-renal manifestations of ADPKD include diverticulosis, abdominal hernias, cysts in liver/thyroid/pancreas/seminal vesicles/etc, mitral valve prolapse, and cerebral aneurysms.
- The biggest risk factor for cerebral aneurysms in patients with ADPKD is a family member with cerebral aneurysms
- DDAVP for uremic platelets works by increasing vwF from endothelial cells
All posts by vmcimchiefs
Morning Report 11/12/15 APLS and Bilateral PEs
- Diagnostic Criteria for APLS: Need ONE lab criteria (confirmed 12 weeks apart) and ONE clinical criteria.
- LAB Criteria: B2 Glycoprotein, Anti-Cardiolipin antibody, or lupus anticoagulant (as measured by prolonged DRVVT which does not correct with a mixing study)
- CLINICAL Criteria: Any Thrombosis (venous/arterial) OR fetal loss/miscarriage
- APLS can be a primary disorder or secondary to other disease (usually Lupus)
- Clinical Features of APLS: 50% have prolonged PTT, 20% with livedo reticularis, cardiac valvular disease (MR), 32% DVT, 13% stroke, 7% hemolytic anemia
- Massive PE refers to PE causing hemodynamic instability (SBP < 90) while submassive PE refers to PE causing right heart strain without hypotension
- Right heart strain from PE: Look for signs of right ventricular hypertrophy and dilatation on EKG, Echo. McConnell’s sign on ECHO is RV hypokinesis with apical sparing
Resident Report 11/9 – Rheumatoid Arthritis
Teaching Pearls:
- Average Age 30-55 years old; F:M ratio 3:1
- Symmetric polyarthritis
- Morning stiffness >1 hour that improves with activity
- OA worsens with activity
- Joint Involvement:
- Almost always involves MCP, PIP, wrist, MTP
- Spares the DIP and lumbar spine
- Think of OA with DIP involvement
- Can occasionally affect large joints
- Swan Neck Deformity
- Boutonniere deformity
- Ulnar Deviation
- C1-C2 subluxation (Atlanto-axial instability)
- This specifically can also be seen in Downs syndrome
- Peri-articular osteopenia
- RA is an independent risk factor for pre-mature coronary artery disease
- RA + pancytopenia + splenomegaly = Felty Syndrome
- RA is a systemic disease that can affect multiple organs. Can be a cause for secondary amyloidosis.
- Amyloidosis – deposition disease that clinically affects the kidneys, liver, and heart.
- Kidney – can lead to nephrotic syndrome
- Hepatomegaly
- Restrictive cardiomyopathy
- Thickening of tongue – lateral scalloping seen on exam
- Waxy skin
- Coagulopathy – amyloid protein causes binding to factor X
- Neuropathy
- GI – causing a malabsorptive syndrome
- Diagnosis requires abdominal fat pad biopsy with Congo red stain to check for apple-green birefringence.
Morning Report 11/4 – CREST and Dermatomyositis
Teaching Pearls:
- Clinical Features of CREST syndrome
- Calcinosis of soft tissue, Raynauds phenomenon, Esophageal dysmotility, Sclerodactyl, Telangiectasia
- Diffuse Cutaneous Systemic Sclerosis (dcSS)
- Skin Findings – Extends past elbows and knees from hands and feet, respectively. Can be seen along torso and face/neck
- Antibody – anti-Scl-70
- Pulm manifestation – interstitial lung disease
- Associated with sclerodermal renal crisis
- Not associated with CREST
- Limited Cutaneous Systemic Sclerosis (lcSS)
- Skin Findings – hands/feet, distal to elbows and knees. Face and neck
- Antibody – ANA centromere pattern
- Pulm manifestation – pulmonary hypertension
- Not associated with sclerodermal renal crisis
- Associated with CREST
- Dermatomyositis
- Heliotropic rash, shawls and V sign, gottron’s papules. Mechanic hands
- Classically associated with proximal muscle weakness
- Elevated CK and aldolase.
- Other studies to consider: EMG and muscle biopsy (definitive diagnosis)
- Associated with anti-Jo-1 antibody (anti-synthetase syndrome)
- Higher association with ILD and worse prognosis
- Higher association with malignancy.
- Colon, breast, ovarian, prostate, etc.
- Few case reports have found an association with oropharyngeal dysphagia, and seems to suggest a poor prognosis sign.
- Serologic Studies/Associations
- Anti-centromere pattern of ANA – lcSS
- Anti-dsDNA Ab – SLE
- Anti-smooth muscle Ab – autoimmune hepatitis
- Anti-La/SSB antibody – Sjogrens, neonatal SLE
- Anti-RNP antibody – Mixed connective tissue disease
- Antihistone antibody – drug induced lupus
- Anti-Scl-70 Ab – dcSS
- Anti-Ro/SSA antibody – Sjogrens, neonatal heart block
- c-ANCA – Wegeners granulomatosis
- p-ANCA – Churg Strauss, microscopic polyangitis
- Anti-Jo-1 Ab – dermatomyositis/polymyositis/anti-synthetase syndrome
- Anti-CCP Ab – Rheumatoid arthritis
Morning Report 11/3 – Hyponatremia
Teaching Pearls:
- Can be categorized into the following:
- Hyperosmolar
- Hyperglycemia, mannitol use
- Iso-osmolar
- Hypertriglyceridemia, hyperparaproteinemia
- Hypo-osmolar
- Hyperosmolar
- Hypo-osmolar hyponatremia can be divided into different categories based on volume status:
- Hypovolemic
- GI losses, diuretic use, blood loss
- ↓↓salt/↓H2O
- Urine osm >100mOsm/L
- Urine Na <20 mmol/L
- Euvolemic
- siADH, psychogenic polydipsia, adrenal insufficiency, hypothyroidism, low solute intake (tea toast diet or beer potomania)
- Salt/↑H2O
- siADH
- Urine osm >100mOsm/L
- Urine Na >40 mmol/L
- Psychogenic polydipsia
- Urine osm<100mOsm/L
- Urine Na >20mmol/L
- Hypervolemic
- CHF, nephrotic syndrome, cirrhosis
- ↑Salt/↑↑H2O
- Urine osm >100mOsm/L
- Urine Na <20mmol/L
- Hypovolemic
- Hypothyroidism presents as a hypoosmolar euvolemic hyponatremia.
- Can present with a clinical picture and urine studies similar to siADH
- Can also present as a picture of CHF.
- Often these patients have myxedema coma.
- Theorized that the decreased cardiac output leads to decreased glomerular filtration, leading to poor excretion of free water.
- Adrenal insufficiency commonly presents with hyponatremia, hyperkalemia, and metabolic acidosis.
- Low solute diet (tea toast diet and/or beer potomania)
- Kidneys can dilute urine to as low as 50mOsm/L.
- If intake of solute is very low, then it limits the amount of free water that can be excreted.
- For more teaching points, check out the hyponatremia section on http://www.professorebm.com.
Morning Report 11/2 – Esophageal Variceal (EV) Bleeding
Teaching Pearls:
- Esophageal varices are seen in roughly 50% of patients with cirrhosis.
- About 33% of patients with cirrhosis and esophageal varices will have at least one clinical presentation of esophageal variceal (EV) bleeding.
- Mortality of 15-20% associated with each episode of esophageal bleeding event.
- EV bleeding comprises of 33% of all cirrhosis-related deaths.
- Risk of EV bleeding correlates with size of varices and other characteristics such as nipple sign and red wales sign.
- Pre-primary prophylaxis – Management of cirrhotic patients without esophageal varices
- Management focuses on treating the underlying cause of cirrhosis.
- Screening occurs ~2-3 years.
- Primary Prophylaxis – Management of cirrhotic patients with EV but no clinical history of GI bleed.
- Medical management with beta blockers
- Performed in those with medium-large varices, or small varices with red wales/nipple sign.
- Esophageal band ligation
- Performed in those with large varices
- Continued Monitoring
- Those with small EV without red wales/nipple sign.
- Medical management with beta blockers
- Immediate interventions to consider in patients with suspected EV bleeding:
- At least 2 large bore PIVs (16 or 18G) or central line
- Fluid resuscitation
- Type and screen blood
- Monitor hemodynamics
- Start protonix (bolus and gtt) and octreotide (bolus and gtt)
- Start ceftriaxone for SBP prophylaxis
- Pantoprazole
- PPI will increase the pH of the gastric lumen to 5-6 from 1-2.
- pH changes help with improving clot formation
- Octreotide
- Works by inhibiting endogenous substances – leads to splanchnic vasoconstriction, decreasing portal flow, leading to decreased portal pressures.
- SBP Prophylaxis Conditions
- History of SBP
- Cirrhosis with GI bleed
- Ascitic TP <1
- Management of gastric varices differ from esophageal varices.
- Cyanoacrylate injection and/or TIPS
Morning Report 10/28 – PFTs
Teaching Pearls:
- FEV1/FVC Ratio <0.7 suggestive of obstructive parenchymal disease
- DLCO – ability for gas to diffuse across alveolar capillary membrane. CO (inhaled) – CO (exhaled). CO has a high affinity for Hb. If CO (exhaled) is higher than expected, DLCO is low and this is suggestive of diffusion problem.
- False Positive
- Anemia
- Pulmonary hypertension
- False Negative
- Pulmonary hemorrhage
- False Positive
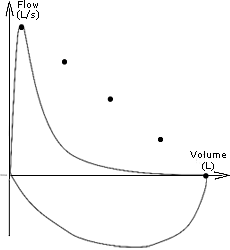
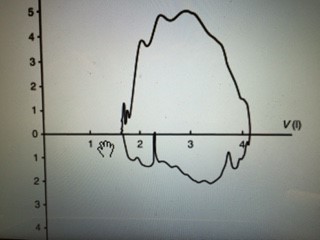
- Pulmonary Function Tests
FEV1 FVC FEV1/FVC DLCO TLC RV F-V Emphysema Decrease Decrease/No change <70% Decrease Normal/increase Normal/increase C Chronic Bronchitis Decrease Decrease/No change <70% Normal Normal/increase Normal/increase C ILD Normal/Decrease Normal/Decrease Normal/Increase Decrease Decrease Decrease A Tracheal stenosis Decrease Decrease/normal Decrease Normal Normal Normal B Resp muscle weakness Decrease Decrease Normal Normal Decrease Increase D A.

B.

- C.

- D.



10/27/15 Morning Report SLE
Teaching Pearls:
- ANA negative lupus, check SSA/SSB which are associated with neonatal lupus and congenital heart block
- ANA positive in 99% of patients with lupus, but low specificity
- double stranded DNA antibodies are used to monitor disease severity in lupus
- check C3, C4, and double stranded DNA to work up possible lupus flare
- Drug induced lupus: Look for positive ANA and anti-histone antibodies. Also look for exposure to procainamide, hydralazine, chlorpromazine, PTU, phenytoin, minocycline, and TNF inhibitors.
| Steroid | Duration | Equivalent Dosing |
| Dexamethasone | Long-acting | 1 mg |
| Methylprednisolone | Intermediate-acting | 4 mg |
| Prednisone | Intermediate-acting | 5 mg |
| Hydrocortisone | Short-acting | 20 mg |
10/22/15 Morning Report Hyperthyroidism
- Pathophysiology of T4 secretion: TSH secreted in the anterior pituitary and stimulates the TSH receptor in the thyroid to secrete thyroid hormone
- Clinical presentation of Hyperthyroidism: Hyperdefecation (not diarrhea), osteoporosis, oligomenorrhea in pre-menopausal females, hair changes, palpitations, arrhythmias
- Etiologies of hyperthyroidism
- Grave’s Disease (most common cause of hyperthyroidism)
- Destructive thyroiditis (subacute, silent, postpartum)
- Multinodular Goiter/Toxic Adenoma
- Medication-induced (amiodarone, lithium, IFN-a, etc)
- Factitious
- Antibodies
- Anti-TPO and anti-thyroglobulin Ab seen with Hashimoto’s Disease (hypothyroidism)
- TSI (thyroid stimulating immunoglobulin) and TBII associated with Graves Disease.
- TSI binds to TSH receptors on thyroid gland, stimulating production of thyroid hormone.
- TSI also binds to TSH receptors located on fibroblasts, stimulating proliferation and glycosaminoglycan production in retro-orbital space.
- Clinical Presentation specific to Graves include pretibial myxedema (5% patients with Graves), exophthalmos (25% of patients with Graves)
- Work-up of Hyperthyroidism
- If evidence for Graves Disease, then GD likely diagnosis.
- Evidence of nodules on physical Exam:
- If None: Perform RAI uptake scan and antibody studies.
- If increased uptake, elevated thyroid hormone due to over-synthesis
- If diffuse uptake, think Graves Disease
- If patchy uptake, think toxic multinodular goiter
- If decreased uptake, think of factitious or destructive causes (subacute, silent, postpartum.
- If increased uptake, elevated thyroid hormone due to over-synthesis
- If Present: Get RAIU scan and thyroid ultrasound to distinguish TNG vs TA and/or evidence of cold nodules. Check for any concerning factors for thyroid cancer.
- If None: Perform RAI uptake scan and antibody studies.
- Thyroglobulin: Precursor to thyroid hormone production. Combined with iodine to produce T4.
- May be used to differentiate factitious vs destructive thyroiditis, surveillance for thyroid cancer.
- Treatment Options:
- Thionamides – Methimazole versus PTU
- Watch for drug rash and/or agranulocytosis
- Radioactive iodine ablation
- Do not use in patients with Graves Disease with severe ophthalmopathy as this can worsen symptoms.
- Surgery
- Thionamides – Methimazole versus PTU
| Grave’s Disease | Multinodular Goiter | Subacute Thyroiditis | |
| Clinical Course/Exam
|
Exophthalmos
Pre-tibial Myxedema |
Hyperthyroid symptoms
Palpable nodules |
Preceded by URI sx, Pain around the neck, pain with palpation, initially hyperthyroid (6 weeks) but progresses to hypothyroid (6 weeks), then normalizes |
| Diagnosis Tests
|
Low TSH
High Free T4 TSI RAIU |
TSH/T4
RAI Thyroid US |
TSH, Free T4
RAI – low uptake Thyroid US – diffuse enlargement |
| Treatment
|
PTU
Methimazole (don’t use in 1st trimester of pregnancy). Watch for agranulocytosis. RAIA, then will require Surgical. Don’t use RAIA for patients with exophthalmos. |
If compressive sx (dysphagia, etc) then surgery
If no compressive symptoms, can treat with RAIU. Toxic patients can also be treated with thionamides |
NSAIDS, supportive
Then Prednisone if poor response Symptomatic treatment, such as propranolol or beta blockers Thionamides not indicated |
Intern Report 10/20 – Bloody Diarrhea
Teaching Pearls
- Duration of Diarrhea
- Acute < 14 days
- Chronic >4 weeks
- Types of Diarrhea
- Secretory
- Stool osmole gap <50
- Osmotic
- Stool osmole gap >100
- Inflammatory
- Evidence of blood and/or mucoid stools
- Malabsorption
- Protein-losing enteropathy
- CHO malabsorption
- Fat malabsorption
- Secretory
- Bacterial Causes of Blood Diarrhea
Source Presentation Complications Treatment STEC (EHEC) Uncooked hamburger meat. Fecal-oral route
Abd pain with bloody diarrhea +/- fever HUS No antibiotics indicated; supportive care Shigella Shellfish, fecal oral route Dysentery (bloody mucoid stools), tenesmus, fever, abdominal pain Reiters Disease Flouroquinolone; 3rd generation cephalosporin Salmonella Undercooked raw eggs, chicken, fruits Fever, abdominal pain, occult/overt bleeding Bacteremia, aortitis, osteomyelitis in those with sickle cell disease Only treat when symptoms are severe Campylobacter Poultry Occult bleeding Reiters disease, Guillain-Barre Syndrome Treat only if severe with macrolides
