
Carriann presented the case of a young woman with HIV (CD4 250 off ARVs) and prior syphilis s/p treatment five years ago who presented with constitutional symptoms and diffuse rash involving the palms and soles, found to have RPR 1:256 consistent with secondary syphilis!
Clinical Pearls
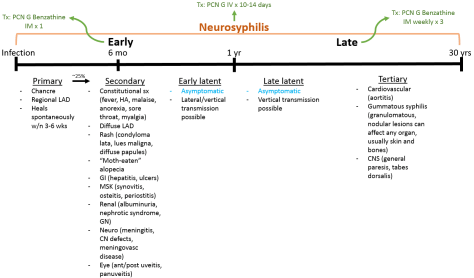
- Lues maligna or malignant syphilis is a rare manifestation of secondary syphilis in immunocompromised individuals and presents as an ulceronodular rash.
- Syphilitic hepatitis is seen in ~10% of patients with secondary syphilis and presents as predominantly elevated alkaline phosphatase with normal or mildly elevated transaminases.
- Neurosyphilis can occur at any point after infection with syphilis!
- Treatment success is defined as a four-fold drop in nontreponemal titers (ie RPR).
Diagnosis:
Keep in mind the following principles:
- Treponemal tests remain positive long-term
- Non-treponemal tests can become negative after treatment. They are useful for treatment monitoring because they can be quantitative
- Both tests can be falsely negative early in disease course so repeat tests if clinical suspicion remains
- Screening algorithm
Treatment monitoring:
- Jarisch-Herxheimer reaction is a self-limited condition that can occur in ~10-35% of patients within 24 hours of treatment with antibiotics.
- A four-fold decline in titers (2 dilutions) is considered treatment success.
- Monitor titers q 6-12 months post treatment. Increasing titer is concerning for treatment failure, neurosyphilis, or reinfection!
