
Thanks to Connie for presenting a case of a young man with chronic bloody diarrhea, abdominal pain, and fever, found to have a new diagnosis of severe Ulcerative Colitis.
Clinical Pearls
- Acute diarrhea requires work up in anyone >65, immunocompromised, blood in stools, fever, severe abdominal pain, recent antibiotics, known or suspected IBD, risky jobs like food handler, or recent travel.
- Fecal calprotectin can help distinguish inflammatory from non-inflammatory diarrhea and is a more sensitive and specific marker than fecal leukocytes.
- 5-ASA based drugs are generally more effective in the colon so their primary role is in the treatment of Ulcerative Colitis or Crohn’s Colitis.

Disease severity in IBD:
- Mild: <4 stools/day, no systemic toxicity
- Moderate: 4-6 stools/day, no systemic toxicity
- Severe: >6 stools per day, systemic toxicity
- Fulminant: >10 BMs per day, continuous bleed, systemic toxicity
Key distinctions between UC and CD:
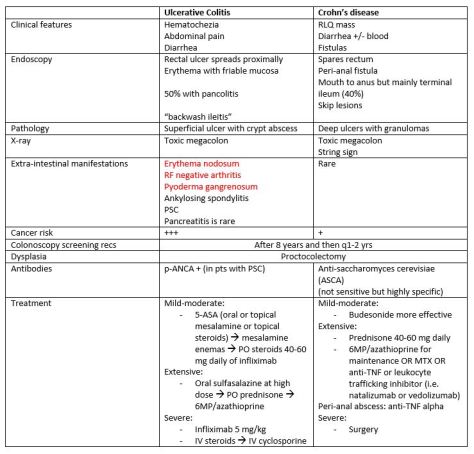
Items in red in the table above correlate with disease activity.
Before initiating immunosuppression:
- Check PPD/quantiferon
- Hepatitis serologies
- Administer routine live vaccines
- Check TPMT level (to assess phenotype for bone marrow suppression secondary to 6MP). If TPMT level low, do not give 6MP!
