
Thanks to Barnie for presenting the case of a middle-aged woman who was admitted with acute onset of SOB, found to have submassive PE.
Clinical Pearls:
- Risk stratification tools are helpful in estimating the pre-test probability of PE. The best and most validated is Wells criteria.
- YEARS items is a newer tool that was studied in an RCT in the Netherlands and found to lower the number of CTPA scans ordered by 14% without a significant impact on rates of missed PE diagnoses.
- For patients at low risk of PE according to Wells, PERC is useful in ED or outpatient setting to rule out PE without ordering a d-dimer (see graphic below).
- Age-adjusted d-dimer is age x 10 for patients older than 50 years. This accounts for the increase in d-dimer baseline related to aging. ADJUST-PE trial showed that age-adjusted d-dimer leads to higher specificity without subsequent VTE.
- Studies have shown an 11.6% reduction in CTPA scans with the use of this correction factor without an appreciable increase in missed diagnoses of PE.
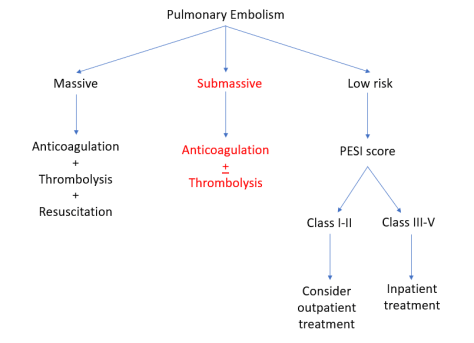
- Think of PE in three broad categories:
- Massive PE = hemodynamically unstable ⇒ anticoagulation + thrombolysis
- Submassive PE = hemodynamically stable + RV strain ⇒ anticoagulation + thrombolysis
- Low risk PE = hemodynamically stable, no RV strain ⇒ anticoagulation. Use the PESI score to determine if your patient can be treated outpatient.
- Remember that the most common EKG finding in PE is normal sinus rhythm! The most common abnormal EKG finding is sinus tachycardia. S1Q3T3 pattern is only seen in 10% of patients with PE.
Diagnosis:
Suggested algorithm for diagnostic work up of suspected PE:
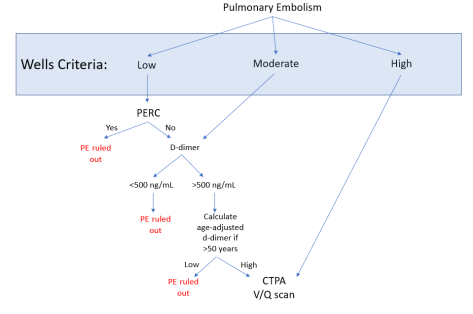
Remember that the scoring tools above are only there to add to your clinical judgment, not replace it!
Recent study in the Lancet looked at the utility of a different diagnostic algorithm, using the three most predictive items on Wells together with d-dimer. Compared to Wells, this diagnostic tool led to a 14% reduction in unnecessary CTPA!

Treatment:
- Remember that clot burden does not factor into the treatment categories of PE. Low clot burden in a patient with baseline cardiopulmonary disease can still lead to hemodynamic compromise and would be considered massive PE.
- Submassive PE treatment is an area of much debate. A famous trial (PEITHO trial) in 2014 randomized 1006 patients to receive heparin + placebo vs heparin + tenecteplase (European version), and found a >50% reduction in combined death and cardiovascular collapse at 7 days but a > four-fold increase in risk of major bleed including intracranial hemorrhage. Subsequent meta-analyses (and this one) found that the risk of major bleeding was highest in people >65 years of age. So treatment decisions here are tricky and require consulting multiple services!
Signs of RV strain:
- EKG findings:
- S1Q3T3: this is a sign of cor pulmonale and can be seen in a number of conditions in addition to PE
- Bronchospasm (really bad asthma)
- ARDS
- Pneumothorax
- S1Q3T3: this is a sign of cor pulmonale and can be seen in a number of conditions in addition to PE
- Echo findings:
- Elevated RVSP
- Septal bowing
- McConnell’s sign (regional wall motion abnormality sparing the RV apex)
- Not sensitive but helpful in distinguishing RV strain due to chronic pulmonary HTN from RV strain due to acute PE
- Increased RV size
- Decreased RV function
- Tricuspid regurgitation
- Labs
- Elevated troponin
- Elevated BNP
