
Thanks Brandan for presenting an elderly lady who developed sudden onset headache, CN3 palsy, and bitemporal hemianopia. She had a CTH that was unremarkable the day before, and a repeat CT found a large pituitary “mass,” and MRI was concerning for pituitary apoplexy!
This case demonstrates a few important concepts:
Visual Field Pathology (commonly tested!)
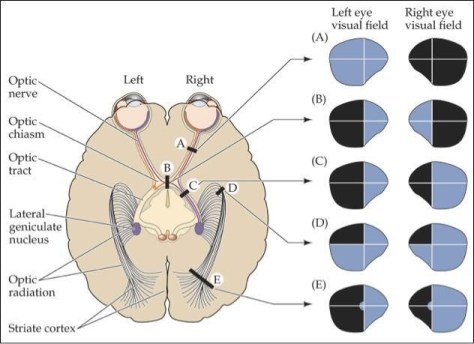
A: Optic Nerve pathology or structural pathology leading to complete blindness in one eye, i.e. trauma, optic nerve neuropathy, optic neuritis (i.e. MS)
B: Bitemporal hemianopsia= optic chiasma pathology until proven otherwise.
C: Homonymous hemianopsia: Optic tract pathology
D: Homonymous quadrantanopsia: Optic radiation, think occipital lobe pathology
Oculomotor nerve palsy (CNIII palsy)
- Findings: Down and out on the affected eye.
- Physiology: Lacteral rectus, with CN VI innervation, remains intact and not opposed by the medial rectus which is innerved by CN III. Down because the superior oblique (innerved by CN IV) is unopposed by the paralyzed superior rectus, inferior rectus, and inferior oblique
- DDx:
- Ischemic (affects somatic fibers over parasympathetic, typically spares the pupils)
- Inflammation,
- Infection
- Tumors (mass effect so both somatic and parasympathetic fibers are typically affected)
- Demyelinating disease
- Autoimmune
- Cavernous sinus thrombosis (don’t miss this!)
Pituitary apoplexy: A Medical Emergency!
- Pathophysiology:
- Hemorrhage or infarction of the pituitary gland usually involving a pituitary adenoma, and occasionally it may be the first manifestation of a pituitary adenoma.
- Risk factors:
- HTN, surgeries, coagulopathies, certain meds (i.e. VKA, DOACs, antiplatelets)
- Presentation:
- Sudden onset headache, vomiting, encephalopathy, visual field defect, hemodynamic instability (esp with ACTH defects).
- DI is very common in the immediate setting, but as axons in the pituitary die, ADH is released which can lead to SIADH (but only transient until stores of ADH are used up), followed by recovery but it depends on the extent of the damage.
- Management: IVF, hydrocortisone (get labs first)
- Acute secondary adrenal insufficiency is seen in 2/3 of pts, important cause of mortality.
- Acute hypocortisolemia leads to hemodynamic instability
- Inc vasopressin release from posterior pit can lead to fluid and lyte disturbances.
- Any signs of hemodynamic instability: Can do 50-100mg hydrocortisone Q6H or continuous infusion 2-4mg/hr
- Role of surgical management:
- Decision to operate based on whether there is deteriorating level of consciousness, severely reduced visual acuity, or presence of visual field defects.
- Otherwise, medical management with corticosteroids, monitoring, re-evaluation is recommended.
- Vision outcomes: Conflicting data on medical vs surgical management.
- Pituitary function outcomes: No difference b/w surgical vs medical management
- Acute secondary adrenal insufficiency is seen in 2/3 of pts, important cause of mortality.
Please refer to this paper for a detailed read on pituitary apoplexy!
