
Thanks to Dr. Szumowski for sending us the case of a middle aged man who presented with acute L knee swelling and pain one week after a viral URI syndrome, initially concerning for septic joint. His clinical course was complicated by recurrent high daily fevers, a diffuse maculopapular rash, and knee arthrocenteses and joint washes that were clean leading to a diagnosis of Still’s disease!
Clinical Pearls
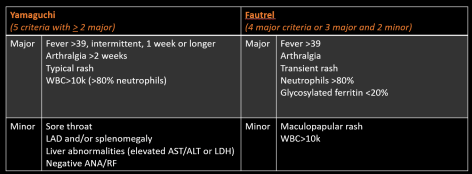
- Still’s disease is a diagnosis of exclusion! Yamaguchi criteria can help with ruling in the diagnosis.
- Still’s remains a multi-systemic disorder of unknown etiology because it’s difficult to diagnose and rare (0.16 cases per 100,000).
- RF and ANA are generally negative but can be positive in <10% of patients with Still’s in low titers.
- ~66% of patients present with sore throat secondary to cricothyroid perichondritis or aseptic nonexudative pharyngitis.
- The disease is often recurrent. Predictors of poor outcome include erosive polyarthritis on presentation and shoulder/hip involvement.
Still’s disease:
- Described in 1897 by George Still, it is a systemic inflammatory disorder of unknown etiology
- Some clarifications on nomenclature:
- Systemic juvenile idiopathic arthritis (sJIA): first presentation <17 years old, previously referred to as Still’s disease
- Adult onset Still’s disease (AOSD): first presentation > 17 years old
- Epidemiology of AOSD:
- 0.16 cases per 100,000
- No sex predominance (F=M)
- Bimodal age distribution with peak between 15-25 and another 36-46 years of age. New diagnosis in patients >60 have been reported.
- Etiology:
- Poorly understood but likely a combination of genetic predisposition, environmental triggers (viruses such as echo, coxsackievirus B4, mycoplasma, yernisnia, lyme, etc), activated innate immunity leading aberrant production of pro-inflammatory cytokines
- Diagnostics:
- High ESR and CRP
- Very high ferritin levels
- Ultimately a clinical diagnosis so it’s important to exclude potential mimickers
- Yamaguchi criteria are the most sensitivity (93.5%)
- Fautrel’s Criteria are the most specific (98.5%)
- Treatment
- Largely empirical since clinical trial data is lacking
- High dose steroids are first line when systemic symptoms predominate
- MTX is second line
- NSAIDs are not good
- Biologic agents for refractory cases (IL1 antagonist anakinra or canakinumab), IL6 antagonist tocilizumab, or TNF inhibitors.
- Course:
- Monocyclic pattern (systemic single episode)
- Polycyclic pattern (multiple episodes, usually <1 /year)
- Chronic pattern (persistently active disease with poly arthritis)

Giacomelli, R. et al. Journal of Autoimmunology. 2018
- Prognosis:
- Poor prognostic indicators:
- Hip and shoulder involvement
- Erosive polyarthritis at initial diagnosis
- Poor prognostic indicators:
