
Thanks to the Human Dx Project for providing us with this fascinating case of a middle aged woman with history of asthma who presented with acute onset of fever and epigastric abdominal pain as well as a chronic progressive cough, found to be febrile, tachycardic, and ill appearing, with E coli bacteremia of unknown source. Further history taking revealed a similar hospitalization several months prior with idiopathic E coli bacteremia. Strongyloides titers were sent and markedly elevated. She was treated with ceftriaxone and ivermectin and made a full recovery.
Clinical Pearls:
- Absence of eosinophilia does not rule out strongyloides. Keep in mind that those presenting with severe illness and hemodynamic instability are commonly in a high cortisol state which can lead to eosinophil apoptosis. Also, in those with history of steroid use (even for short periods of time), eosinophil count can be negative.
- Think of strongy in anyone with the right travel history, older age, malnutrition, HIV, or steroid use.
- Signs and symptoms can be quite non-specific so a high index of suspicion is required to make the diagnosis.
- Think of strongyloides in a patient with history of recurrent GNR bacteremia of unknown etiology!
Strongyloidiasis
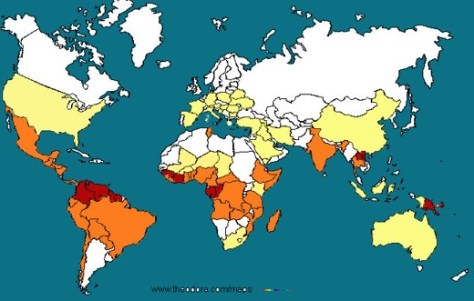
- Higher incidence noted going from yellow to orange to red on the map above
- Epidemiology
- Typically in travelers to endemic areas, immigrants from endemic regions, or anyone with barefoot contact with infested soil.
- Risk factors include older age, malnutrition, HIV, and steroid use
- Signs and symptoms
- Infected people can be asymptomatic or minimally symptomatic for years:
- Could also have mild waxing and waning GI, skin, or pulmonary symptoms for years
- Eosinophilia without symptoms
- Skin: urticarial, larvae currens (see picture below), angioedema, erythroderma

- Pulmonary: chronic cough, hemoptysis, recurrent pneumonia, astham that gets worse with steroids
- GI: upper abdominal pain, duodenitis, diarrhea, anorexia, recurrent enteric GNR bacteremia
- Disseminated disease/hyperinfection syndrome:
- Increased parasite burden due to autoinfection (see picture below)
- Massive dissemination of larvae to lungs, liver, heart, CNS, and endocrine glands
- Can present with septic shock or multiorgan failure
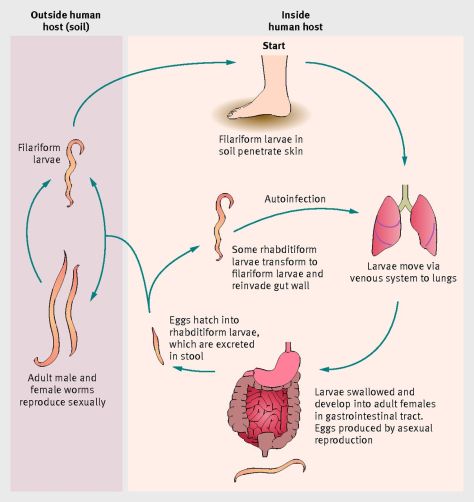
Greaves, D. BMJ 2013; 347:f4610
- Infected people can be asymptomatic or minimally symptomatic for years:
- Diagnosis:
- Stool O&P: <50% sensitive and requires multiple samples due to intermittent shedding
- Serologies: 89% sensitive
- Treatment:
- Ivermectin or albendazole
- Hyperinfection/disseminated disease: above PLUS broad-spectrum antibiotics
Quick review of endemic dimorphic fungi:
- Southwest US ⇒ Cocci
- Ohio & Mississippi River Valley ⇒ Histo
- Southeast/South-central US ⇒ Blasto
- Southeast Asia ⇒ Penicillium
- South America ⇒ Paracocci, histo, blasto, cocci
