Brooke presented a fascinating case of a middle aged man with history of substance use disorder presenting with acute on chronic back pain, weakness, and urinary retention, found to have subacute combined degeneration of the spinal cord from vitamin B12 deficiency due to using >100 canisters of nitrous oxide daily!
Clinical Pearls
- Vitamin B12 deficiency can lead to degeneration of the dorsal and lateral white matter of the spinal cord ⇒ subacute combined progressive weakness, sensory ataxia, paresthesias, spasticity, paraplegia, and incontinence.
- Nitrous oxide use (“Whippits”) inactivates vitamin B12 in the blood, rendering the body effectively vitamin B12 deficient.
- In patients with history of N2O abuse, always check MMA levels with vitamin B12 since the latter is not a marker of functional B12 availability.
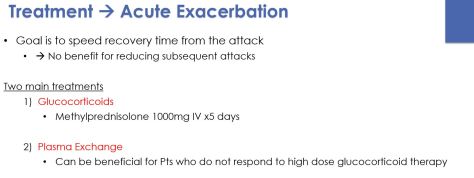
- Treatment involves high dose B12 supplementation and stopping Whippits!
Differential for myelopathies:
- Syringomyelia ⇒ cavitation of central spinal cord resulting in LMN symptoms with sensory changes
- Inflammatory
- Transverse myelitis
- Viral prodrome
- Usually associated with MS or autoimmune diseases
- Typically involves the thoracic cord
- Symptoms develop over hours
- Sarcoid
- Mimics transverse myelitis or tumor
- Praneoplastic syndromes
- Transverse myelitis
- Infectious
- Epidural abscess
- Acute viral myelitis
- Enteroviruses (coxsackie, polio), flaviviruses (WNV, Japaneses encephalitis)
- CMV, VZV, HSV, HCV, EBV (these viruses are less clearly associated)
- AIDS myelopathy
- HTLV-1 myelopathy
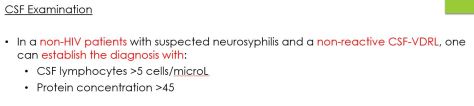
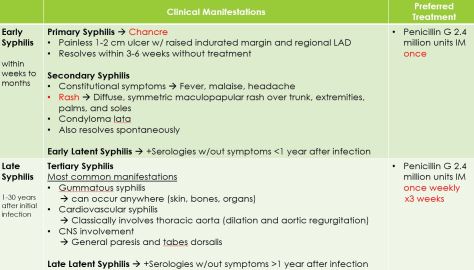
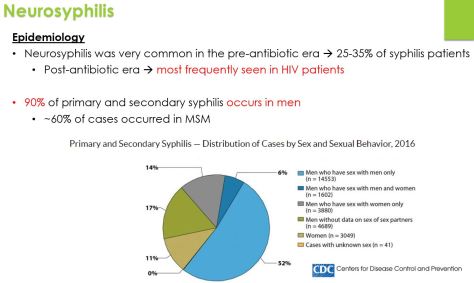
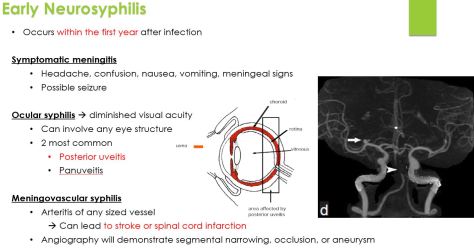
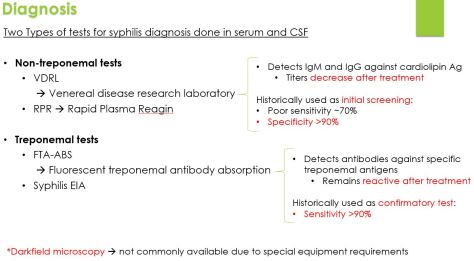
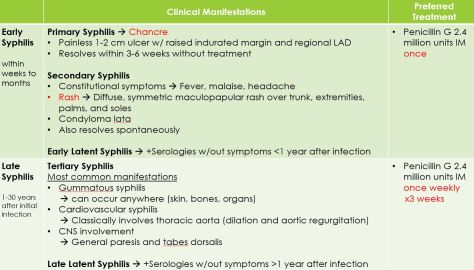
- Syphilis
- Tabes dorsalis (affects dorsal columns)
- TB
- Parasites
- Schistosoma, cysticercosis
- Vascular
- Spinal cord infarction
- Vascular malformations
- Spinal epidural hematoma
- Toxic/metabolic disorders
- Subacute combined degeneration of spinal cord ⇒ degeneration of dorsal and lateral white matter (think Whippits and B12 deficiency!)
- Copper deficiency myeloneuropathy
- Radiation induced myelopathy
- Hepatic myelopathy (purely motor symptoms, lower extremities predominant, in patients with ESLD)
- Decompression sickness myelopathy (in deep sea divers)
- Neoplasms
- Degenerative conditions
- ALS
- Demyelinating diseases
- MS
Inhalant Abuse:
Side effects are broad and include
- CNS effects
- CV: arrhythmias, myocarditis, MI “sudden sniffing death”
- Pulmonary: hypoxia, pneumonitis, hemorrhagic pulmonary edema, PTX from pressurized tanks
- GI: n/v, abdominal cramps, anorexia, hepatotoxicity
- Renal effects: AGMA (with volatile substances), urinary calculi, nephrolithiasis
- Hematologic: aplastic anemia, malignancy (leukemia, lymphoma, MM)
- Derm: “Glue-sniffer’s rash”. Eczematoid dermatitis with erythema, inflammatory changes, and pruritis in the perioral area and midface
- MSK: rhabdo