Primary spontaneous pneumothoax – that which happens without any underlying lung disease – in actuality, most of these patients just have undiagnosed lung disease
Secondary spontaneous pneumothorax – that which happens with known underlying lung disease
Risk factors – tall stature, male sex, Marfan’s, homocysteinuria, thoracic endometriosis, smoking
Clinical presentation – dyspnea, pleuritic chest pain, decreased breath sounds, hyperressonance to percussion, and decreased chest excursion
Patients are able to prevent hypercapnea because of their good lung but cannot prevent hypoxia because the areas of collapsed lung still receive perfusion.
From MKSAP 17:
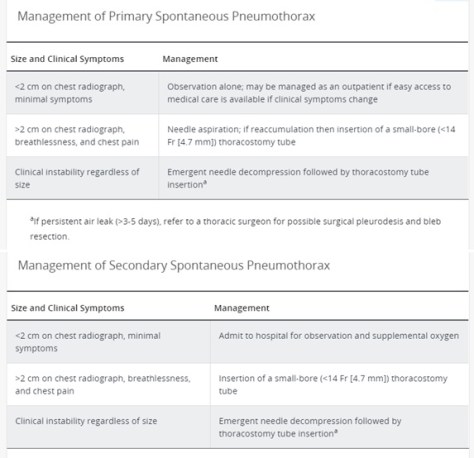
Patients with a primary spontaneous pneumothorax are safe to fly after re-expansion of the lung. Scuba diving is NOT safe even after re-expansion of the lung.
Recurrence rate for primary spontaneous is 23-50% over the first 5 years and 50% in secondary spontaneous pneumothorax.