







All posts by vmcimchiefs
SJS and TEN – 10/19/2017









Varicella Zoster – 10/18/17
Primary infection – chicken pox (lesion at varying stage on the trunk, face, and extremities)
Reactivation – shingles (painful, unilateral rash in a restricted dermatome)
Clinical manifestations – 1) Rash – most common location is thoracic and lumbar dermatomes
2) Acute neuritis – 75% of patients have pain/burning/throbbing prior to onset of rash
Complications in immunocompetent hosts – post-herpetic neuralgia (7.9%), ocular complications (1.6%),, meningitis (0.5%), oticus (0.2%)
Disseminated if > 3 contiguous dermatomes or 2 dermatomes on separate parts of the body
Diagnosis for encephalitis/meningitis – elevated WBC with lymphocytic predominance, elevated protein, positive VZV PCR or IgM
Treatment: IV acyclovir
Vaccines: Age > 60 give live vaccine unless immunosuppressed
VZIG – give to exposed pregnant or immunosuppressed patients
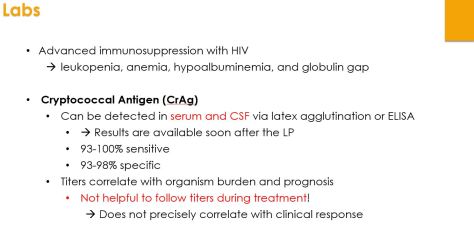
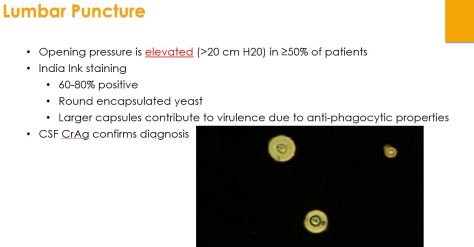
Cryptococcal Meningitis – 10/17/2017





Disseminated Gonococcal Infection – 10/16/17
Epidemiology
- Young (< 40 years old)
- Women (because they are usually asymptomatic)
- 0.5-3% of people infected with N. gonorrheae
- Common cause of acute arthritis in young people
Clinical Manifestations
- 1) triad of tenosynovitis (migratory), dermatitis (painless lesions – usually pustular or vesiculopustular), and polyarthralgias (small or large joints – usually asymmetric)
- 2) purulent arthritis without skin lesions – usually one joint affecting knees, wrist, or ankles
Evaluation
- Clinical suspicion – thorough history of physical
- Blood cultures
- Specimen from mucosal sites – urogenital, rectal, pharyngeal
- Synovial fluid – only positive 50% of the time – NAAT testing better than cultures
Treatment
- Ceftriaxone 7-14 days (can give IM if non-purulent arthritis)
- Remember to co-treat for chlamydia with azithromycin
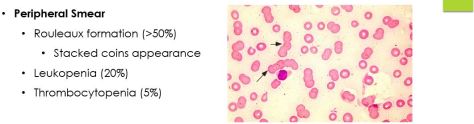
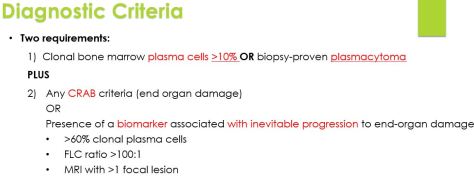
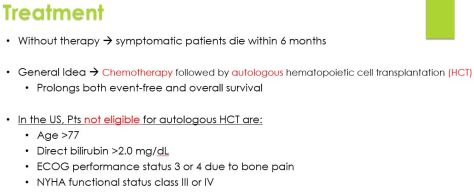
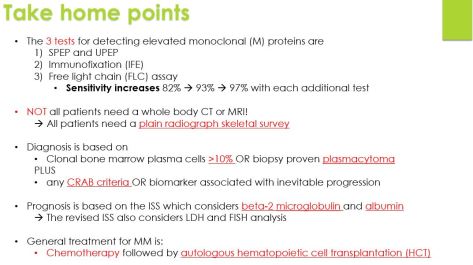
Multiple Myeloma – 10/10/2017






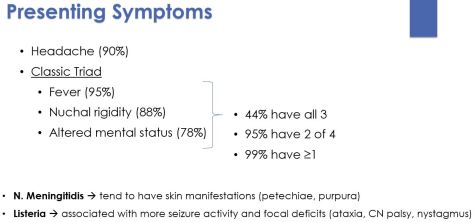
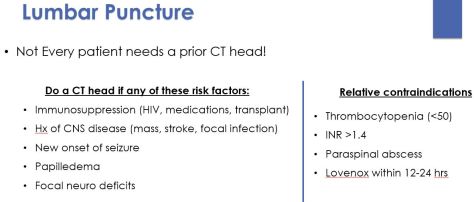
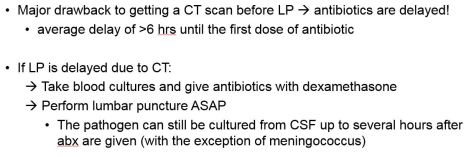
Acute Bacterial Meningitis – 10/03/2017






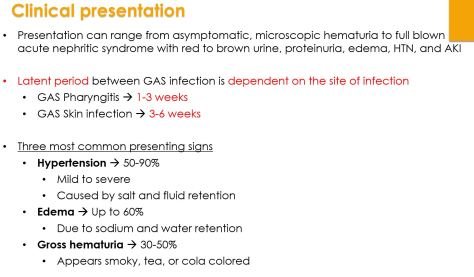
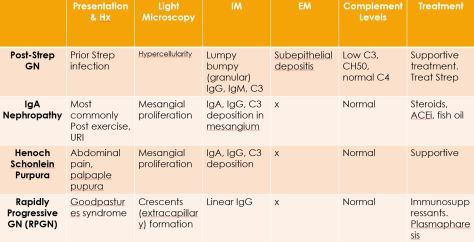
Post-Streptococcal Glomerulonephritis






Dysphagia – 09/19/2017










Critical illness myopathy – 9/20/17
Remember – a lot of this diagnosis can be made with labs and a good physical exam!
Steroid induced myopathy – normal CK and normal DTRs
Critical illness myopathy/neuropathy – elevated CK and decreased DTRs
GBS – normal CK and decreased DTRs
Inflammatory myopathy – elevated CK with normal DTRs
If you have a patient who had inflammatory myopathy and was receiving steroids for treatment and despite a normalization in CK did not have improvement in weakness – wean off the steroids because this likely now became a steroid induced myopathy!
