
Thanks to Amran for presenting an interesting case of a 84yo M with RA on MTX & Prednisone, and an unspecified self-resolving total body rash 1 month prior to presentation, presenting with pain, redness, and vision in both eyes. Detailed fundoscopic exam was consistent with bilateral anterior granulomatous uveitis as well as retinitis, consistent with a panuveitis picture. Initial work up revealed RPR and EIA positivity, his HLA-B27 also returned positive but he has no other findings suggestive of spondylosing arthropathy. His vitreal centesis returned positive for VZV!
In Summary:
- Tertiary syphilis without CNS/ocular involvement
- Panuveitis secondary to VZV
- Incidental HLA-B27 without e/o ankylosing spondylitis
Let’s start off with a basic review of the eye anatomy:
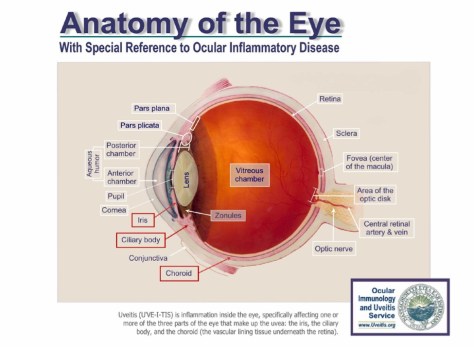
The Uvea consists of the iris, ciliary body, and the choroid. Uveitis is inflammation of any of these structures.
The Standardization of Uveitis Nomenclature (SUN) Working group guidance on uveitis terminology categorizes uveitis anatomically as follows;
- Anterior uveitis; localized primarily to the anterior segment of the eye, involving iris and pars plicata.
- Intermediate uveitis; localized to the vitreous cavity and pars plana, presence of WBC in the vitreous.
- Posterior uveitis; localized to the choroid and retina.
- Panuveitis; inflammation involving anterior, intermediate and posterior uveal structure
Uveitis can be further classified into granulomatous (presence of macrophages, multinucleated giant cells) vs non-granulomatous. A granulomatous uveitis is typically more likely to be an infectious process (although can still be idiopathic or Sarcoidosis).
Etiology of Uveitis
- Infectious:
- HSV:
- Usually unilateral, might have other clues such as presence of vesicles.
- Toxoplasmosis:
- Ocular toxoplasmosis for some reasons occurs more frequently in immunocompetent hosts.
- Lyme Disease
- Syphilis:
- Accounts for less than 1% of cases of uveitis but can affect any part of the eye.
- TB (Yes ocular TB exists!)
- Uncommon in North America, suspect in endemic regions and worsening sx with glucocorticoids.
- CMV:
- Almost exclusively in immunocompromised hosts i.e. AIDS patients.
- CD4 < 50 typically.
- Bartonella (ocular bartonellosis) aka Cat Scratch Disease:
- Typically unilateral, has a characteristic “macular star” on fundoscopic exam.
- West Nile virus
- Ebola (case reports)
- Zika virus
- Varicella Zoster Virus: Can affect any part of the eye
- HSV:
- Non-infectious: Most common = HLA-B27 related arthropathies and reactive arthritis, tends to be unilateral and causes an anterior uveitis picture
- Sarcoidosis
- IBD
- Ankylosing spondylitis
- Relapsing polychrondritis:
- Behcets
- Juvenile idiopathic arthritis
- Psoriatic arthritis
- Reactive arthritis
- TINU (tubulointerstitial nephritis and uveitis) syndrome
- Uncommon, occurs in adolescent/young F, fever, myalgias, anemia, LFT elevation, chronic uveitis, interstitial nephritis.
- MS: Optic neuritis
- Vogt-Koyangi-Harada(VKH)Syndrome:
- Japanese and Hispanics, bilateral panuveitis, neurological/auditory sx
- Penetrating trauma
- Drug-induced:
- Rifbutin, fluoroquinolone, monoclonal ab
- Other conditions that might mimic uveitis
- Retinal tears
- Ischemia
- Leukemia
- Lymphoma
- Ocular melanoma
- Pigmentary dispersion syndrome
- Retinitis pigmentosa
- Retinoblastoma
Management
- Treat underlying cause
- If viral: Anti-virals (acyclovir, valacyclovir), add on topical corticosteroids.
- Non-infectious uveitis: Management typically with topical steroids. If posterior, some have suggested using difluprednate or periocular glucocorticoid injections. Systemic tx is reserve for pts with bilateral disease, inability to tolerate intraocular injections, or systemic conditions i.e. Behcets.
- If refractory to steroids in non-infectious causes, can consider MTX, azathioprine, mycophenolate, cyclosporine, or tacrolimus.
- TNF alpha inhibitors u.e. adalimumab has good evidence in the tx of non-infectious intermediate, posterior, and panuveitis. Can also be considered first line in management of Behcet.
- Sulfasalazine has been shown in a few small studies to prevent HLA-B27 associated uveitis.
Please refer to this previous blog post for more details on tertiary syphilis!
