Morning Report Candida Pyelonephritis – 8/28/17 August 28, 2017 vmcimchiefs Leave a comment Risk factors for systemic candida include immunosuppression, intravascular catheters (TPN), broad spectrum antibiotics Infection is considered systemic once you have positive blood cultures Once you are concerned for systemic infection, make sure to get an Ophthalmology consult to rule out endophthalmitis! Start with an echinocandin for treatment unless you have a UTI, meningitis, or endophthalmitis in which cause you should use an azole medication If you have evidence of Candida glabrata then an azole may not work because there tends to be resistance If you have Candida glabrata meningitis, UTI, or endophthalmitis, you should start with amphotericin until you have susceptibilities Do not treat asymptomatic candiduria unless the patient is neutropenic or had recent urologic procedures done
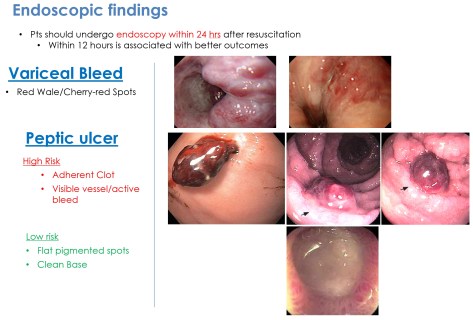
Morning Report Upper GI Bleed 08/08/2017 August 11, 2017 vmcimchiefs Leave a comment Upper GI Bleed = Proximal to ligament of Treitz (suspensory muscle that holds the duodenum) Lower GI Bleed = Distal to ligament of Treitz Factors most predictive of an upper GI source Hx of Melena Hematochezia is usually due to lower GI Bleed, But it can still occur with massive upper GI bleeding! Coffee ground emesis Ratio BUN:Cr >30
Morning Report Status Epilepticus – 08/02/2017 August 2, 2017 vmcimchiefs Leave a comment Do we use Keppra (Levetiracetam) for GCSE? Generally No -> Not FDA approved for status epilepticus. Keppra has weak evidence to support it in the treatment of status More useful in suppressing subsequent seizures after GCSE is controlled