This morning we presented a case of SVC syndrome with complete thrombotic occlusion.
SVC 101
- What is it?
- Obstruction of blood flow through the SVC
- What are the three mechanisms by which this can happen?
- Thrombosis
- Invasion
- Extrinsic Pressure
- How does the body compensate?
- Collateral veins develop to return blood to the heart
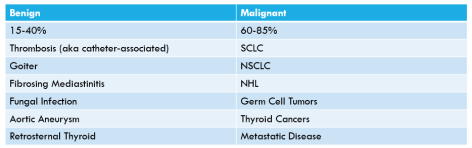
Causes of SVC Syndrome
SVC Symptoms
- Facial and neck swelling
- Chest pain
- Respiratory symptoms
- Neurological manifestations such as head fullness, which may worsen by bending forward or lying own
- Headaches, confusion, audiovisual disturbances
- Cerebral edema can be fatal
- Arm swelling
- Onset of symptoms depends on whether collaterals had a chance to form
Physical Examination
- May see distended chest wall veins
- Pemberton’s sign may be positive
- initially discovered in the context of a goiter, it can also be useful to identify other causes of SVC obstruction
- have the patient raise their arms for two minutes and watch for increasing facial plethora (swelling and redness)
Treatment Options
- Depends on urgency. If emergent, ABCs then straight to endovascular management with pharmacologic thrombolysis/balloon angioplasty/etc +/- stenting
- If non-emergent, can obtain imaging and biopsy and plan treatment course with chemotherapy or radiation
Lastly, check out Radiopedia! It’s a great learning tool and really fun too.