- Risk factors for systemic candida include immunosuppression, intravascular catheters (TPN), broad spectrum antibiotics
- Infection is considered systemic once you have positive blood cultures
- Once you are concerned for systemic infection, make sure to get an Ophthalmology consult to rule out endophthalmitis!
- Start with an echinocandin for treatment unless you have a UTI, meningitis, or endophthalmitis in which cause you should use an azole medication
- If you have evidence of Candida glabrata then an azole may not work because there tends to be resistance
- If you have Candida glabrata meningitis, UTI, or endophthalmitis, you should start with amphotericin until you have susceptibilities
- Do not treat asymptomatic candiduria unless the patient is neutropenic or had recent urologic procedures done
All posts by vmcimchiefs
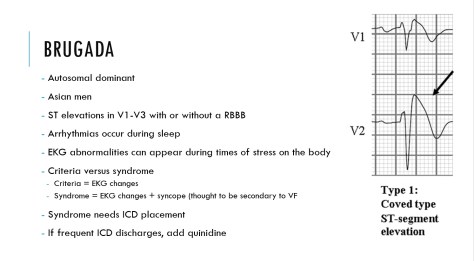
Brugada Syndrome 8/23/17
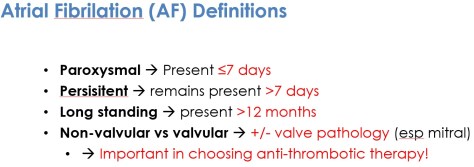
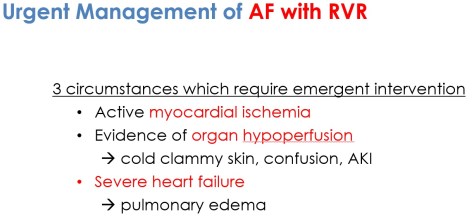
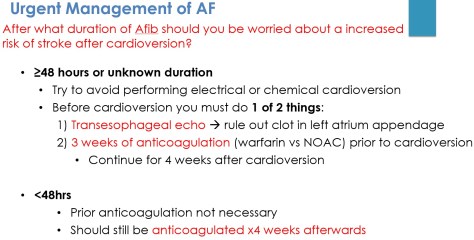
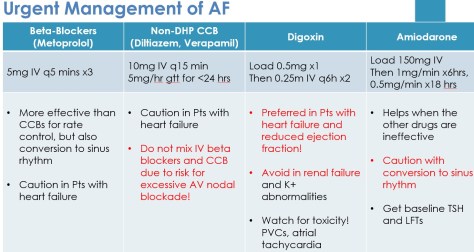
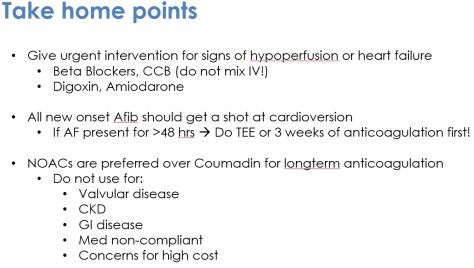
New Onset Afib – 08/15/2017






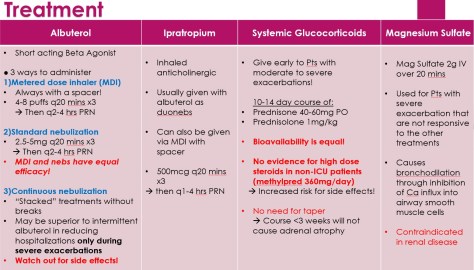
Asthma Exacerbation – 08/10/2017





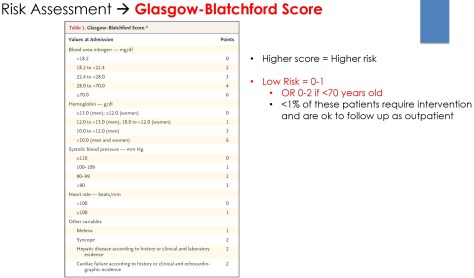
Upper GI Bleed 08/08/2017
- Upper GI Bleed = Proximal to ligament of Treitz (suspensory muscle that holds the duodenum)
- Lower GI Bleed = Distal to ligament of Treitz
- Factors most predictive of an upper GI source
- Hx of Melena
- Hematochezia is usually due to lower GI Bleed, But it can still occur with massive upper GI bleeding!
- Coffee ground emesis
- Ratio BUN:Cr >30
- Hx of Melena



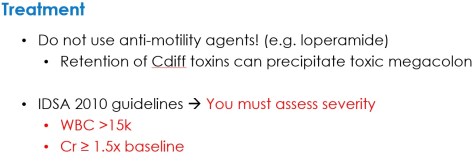
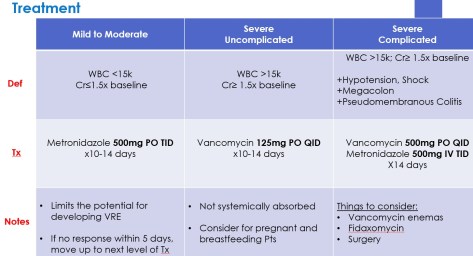
Clostridium Difficile – 07/31/2017




Status Epilepticus – 08/02/2017




- Do we use Keppra (Levetiracetam) for GCSE?
- Generally No -> Not FDA approved for status epilepticus.
- Keppra has weak evidence to support it in the treatment of status
- More useful in suppressing subsequent seizures after GCSE is controlled
- Generally No -> Not FDA approved for status epilepticus.
Leukemia – 8/1/17

Myxedema Coma – 7/27/17
Most common presentation
- Altered mental status
- Hypothermia
- Precipitating event
- **Myxedema and coma do not have to be present**
Physical exam findings
- Hypothermia
- Bradycardia
- Hypotension
- Cool skin
- Diffuse soft tissue swelling without pitting
- Altered mental status
Lab abnormalities
- Hyponatremia
- Elevated CK
- Elevated transaminases
- Hypoglycemia
- Elevated TSH with frankly low T4 level
Treatment
- IV levothyroxine
- Use of T3 is controversial
- Stress dose steroids because of concern for precipitating adrenal insufficiency
- Supportive measures
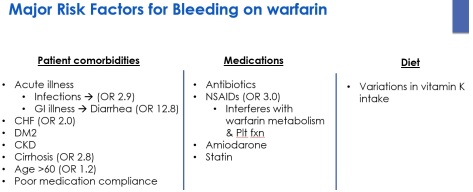
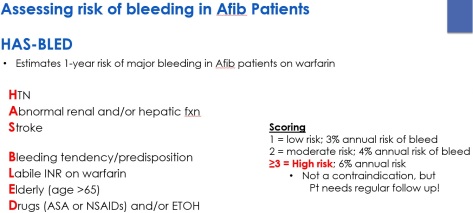
Supratherapeutic INR on Warfarin 07/26/2017
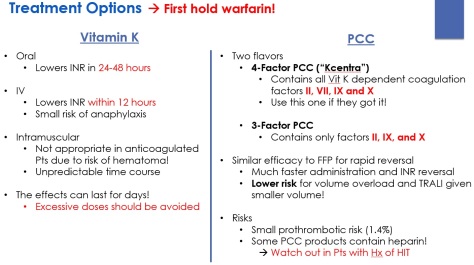
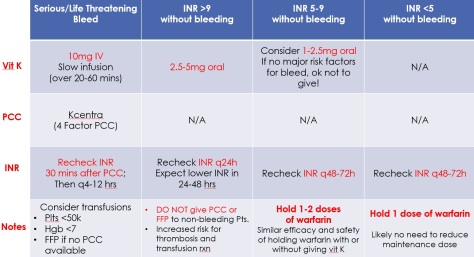
What if there is minimal bleeding?
- There are no set guidelines from ACCP for this situation
- It depends on clinical judgement and the likelihood of progression to severe bleeding
- Extent and site of current bleeding
- Previous bleeding
- Comorbidities
- INR level and trend
- Use a combination of holding warfarin and giving vitamin K as appropriate