Definition: mPAP greater or equal to 25 mmHg at rest
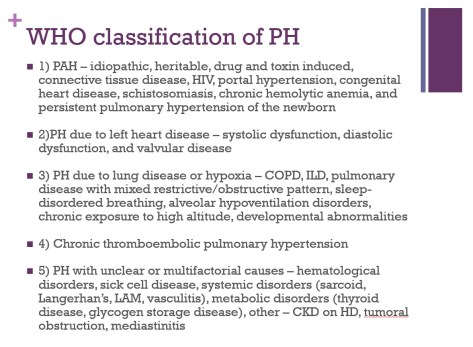
- Can also classify as pre and post-capillary
- Pre-capillary is group 1, 3, 4, 5
- Post-capillary is group 2 and 5
- Combination can be group 2 and 5
- If enough volume overload to cause enough right heart strain to cause intrinsic remodeling then group 2 could cause intrinsic PAH
- Best prognosis is CTEPH if able to surgically remove the clot (usually able to do so in proximal clots)
- Worst prognosis is PAH
- Most common form of group 3 is due to COPD
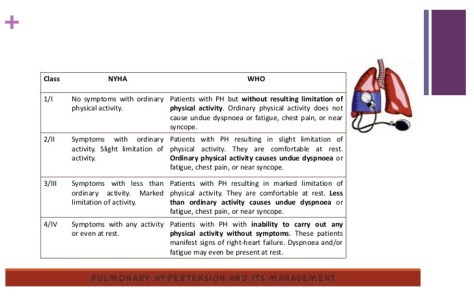
Symptoms
– Most common is dyspnea
– Other symptoms include exertional chest pain due to increased myocardial oxygen demand from enlarged right ventricle and increased pressure, peripheral edema, and anorexia (from hepatic congestion)
Diagnostic evaluation
– Transthoracic echo as screening and if evidence of heart disease then likely group 2
– If no evidence of left heart disease then check PFTs, overnight oximetry, VQ scan, LFTs, HIV, ANA, etc to rule out other etiologies of PH
– Patients only need a RHC for confirmation or if other cause of possible PH does not fit the extent of PH seen
– Vasoreactivity testing – if positive then patient would benefit from CCB
– Positive vasoreactivity test is a drop in mPAP of at least 10 and less than 40 mmHg overall without hypotension or drop in CO
Treatment
– For group 2-5 treat the underlying cause
– If evidence of PaO2 < 60 in group 3 then start oxygen
– Treat with anticoagulation to prevent further clots in CTEPH but only definitive treatment is thrombectomy
– For group 1 – can use vasodilators, anticoagulation (because high risk of PE in these patients), digoxin for right heart contractility, and diuretics for volume management