Thanks to Tim for presenting the interesting case of a middle-aged man with h/o inadequately treated syphilis who presented with neck stiffness worse in the mornings, back pain, and blurry vision, admitted for presumed neurosyphilis. Exam revealed inflammation of T2/T3 joints, L SI joint tenderness, and an inflamed R foot with dactylitis of the 3rd and 4th digits. Further history revealed a recent gonorrhea/chlamydia for which he was treated and HLA B27 positivity consistent with reactive arthritis! He was started on NSAIDs with significant improvement of symptoms.
Clinical Pearls:
- Neurosyphilis is most commonly seen in HIV positive patients and can present at any time after infection.
- Early neurosyphilis occurs within the first year after infection and involves the CNS, meninges, and vasculature
- Neurosyphilis presents with posterior uveitis or pan-uveitis whereas reactive arthritis presents with anterior uveitis
- Late neurosyphilis occurs >10 years after infection and involves the brain and spinal cord parenchyma
- The four main spondyloarthropathies are ankylosing spondylitis, psoriatic arthritis, reactive arthritis, and IBD-related arthritis.
- The genital pathogen most commonly associated with reactive arthritis is chlamydia trachomatis.
- HLA B27 is positive in 30-50% of patients
- Mainstay of treatment is NSAIDs
- Disease typically lasts 3-5 months.
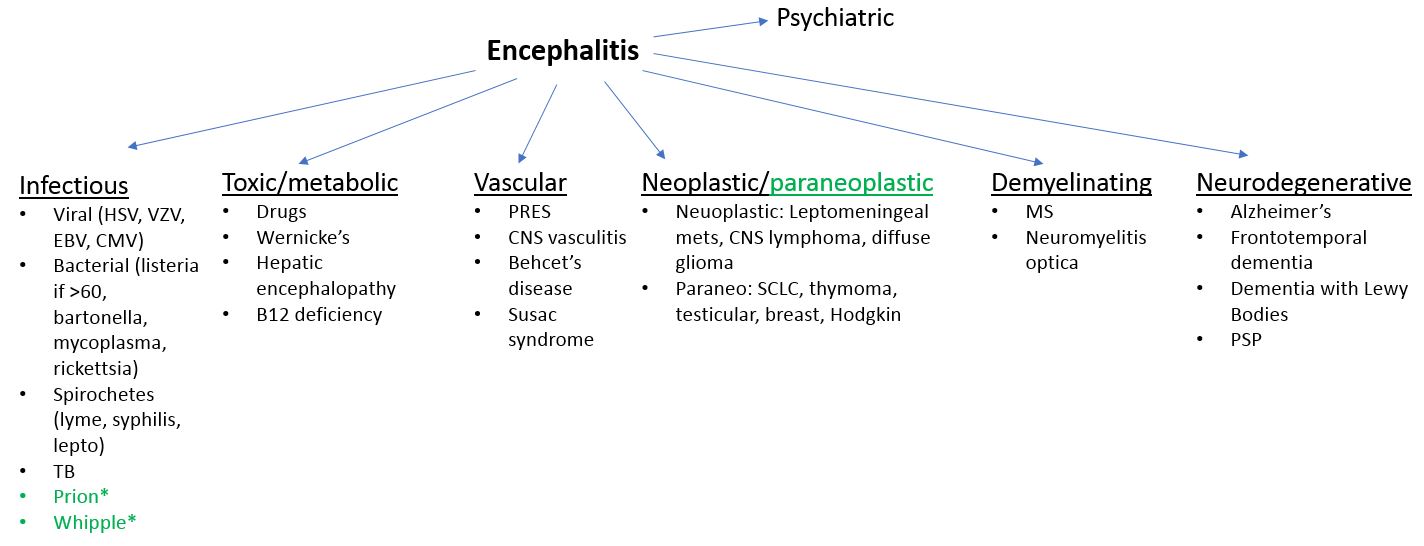
Syphilis

Neurosyphilis manifestations
- Refer to this prior post
- Early (w/n first year of infection)
- CSF, meninges, vasculature
- Symptomatic meningitis
- Ocular syphilis (posterior uveitis, panuveitis)
- Meningovascular syphilis
- Arteritis of any sized vessel which can lead tostroke or spinal cord infarction
- Late
- Brain and spinal cord parenchyma
- General paresis (10-25 years after initialinfection)
- Progressive dementia
- Psychiatric symptoms
- Tabes dorsalis (>20 years after initialinfection)
- CSF may be completely normal
- Affects dorsal columns
- Symptoms
- Sensory ataxia
- Argyll-Robertson pupil
- Lancinating pains
- General paresis (10-25 years after initialinfection)
- Brain and spinal cord parenchyma
- Diagnosis
- Non-treponemal tests (poor sensitivity but highspecificity)
- VDRL
- RPR
- Treponemal tests
- FTA-ABS
- Syphilis EIA
- In an HIV negative patient with suspectedneurosyphilis and a non-reactive CSF-VDRL, one can establish the diagnosis with
- CSF lymphocytes >5 cells/microL
- CSF protein concentration >45
- Non-treponemal tests (poor sensitivity but highspecificity)
Reactive Arthritis
- Epimiology
- Young adults, M:F equal
- Typically follows GI or urogenital infections (several days to weeks after infection)
- Chlamydia trachomatis (most common genital infection associated)
- Yersinia
- Salmonella
- Shigella
- Campylobacter
- E coli
- C diff
- Chlamydia pneumoniae
- Manifestations
- Mono- or oligoarticular pattern of arthritis,often involving the lower extremities, sometimes associated with dactylitis and enthesitis
- The triad of arthritis, urethritis, andconjunctivitis is only present in a subset of patients (formerly called Reiter’s syndrome)
- Ocular manifestions: conjunctivitis, less frequently anterior uveitis, episcleritis, and keratitis.
- Other:
- Skin: keratoderma blennorhagica, erythema nodosum
- Circinate balanitis
- Nail changes resembling psoriatic arthritis
- Lab
- E/o of antecedent or concomitant infection
- Elevated acute phase reactants
- Positive HLA-B27 (present in 30-50% of patients)
- Inflammatory synovitis
- Imaging consistent with enthesitis or arthritis
- Treatment
- Treat any ongoing concurrent infection
- NSAIDs (first line)
- Steroids (if refractory to NSAIDs)
- DMARDS (for chronic reactive arthritis)
- Anti-TNF (last resort)
- Prognosis
- Duration is typically 3-5 months
- >6 months duration is considered chronic reactive arthritis
- Most remit completely or have little active disease w/n 6-12 months after presentation
- 15-20% may experience more chronic persistent arthritis
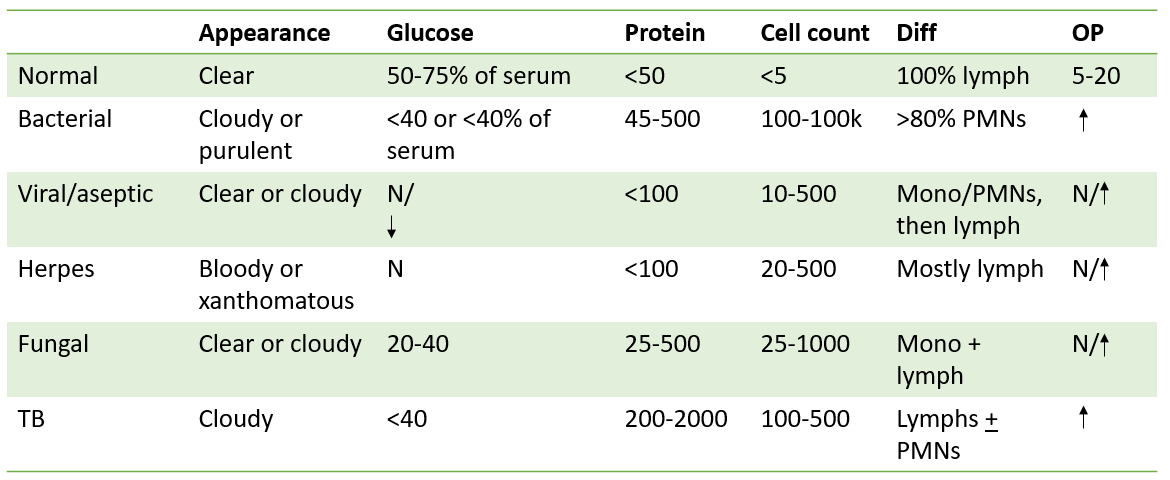



 Image adapted from Derm 101
Image adapted from Derm 101