Thanks to Naina for presenting the case of an elderly man presenting with acute onset of n/v, and abdominal pain, found to have anemia and AKI, with work up revealing small cell cancer of the bladder causing ureteral obstruction with mets to the lymph nodes, liver, lung, and bone, hospitalization complicated by TLS prior to onset of chemo and contrast induced nephropathy.
Clinical Pearls
- Bladder cancer is the most common malignancy of the urinary system and urothelial (transitional cell) carcinoma is the culprit >90% of the time. Less common subtypes include squamous, adeno, small cell (our patient), and sarcoma.
- Unexplained hematuria in anyone >40 years is bladder cancer until proven otherwise!
- CT urography is the diagnostic imaging of choice in the work up of hematuria.
- Diagnosis of bladder cancer is often delayed due to similarity of symptoms with other benign disorders. However, majority of cases are still caught in stage 0-1 (muscle non-invasive disease) with overall good prognosis.
Bladder cancers:
- Epidemiology
- Most common malignancy of the urinary system, 3-4 x more common in men but women are usually diagnosed with more advanced disease and have a higher mortality rate.
- Median age at diagnosis is ~70
- Incidence has increased by more than 50% during the past 20-30 years.
- Types:
- Urothelial (transitional cell) carcinoma is the predominant histologic subtype in the US and Europe (>90% of all bladder cancers) and can arise in renal pelvis, ureter, or urethra
- Other: squamous, adeno, small cell, sarcoma
- Degree of invasion:
- Superficial (non-muscle-invasive)
- Muscle-invasive
- Metastatic
- Clinical presentation
- Painless hematuria
- Irritative voiding symptoms (frequency, urgency, dysuria) – only in 30% of patients
- Sometimes metastases cause the initial symptoms that lead to diagnosis (as in our patient)
- Most cancers eventually become symptomatic
- Diagnosis: often delayed due to similarity of symptoms to other benign d/o
- Urine cytology >98% specific, 12-64% sensitive based on grade of tumor
- Imaging
- CT favored over IVP
- TURBT done for diagnosis and staging
- DDx
- Hematuria from enlarged prostate
- Pregnancy
- Cystitis
- Prostatitis
- Passage of renal calculi
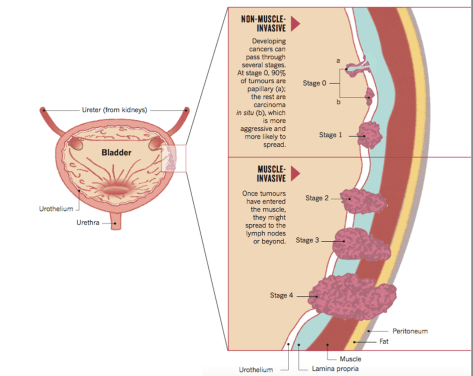
Source: Nature Outlook.
- Management
- Over 50% of people diagnosed with non-invasive disease develop recurrence
- Assess performance status with Karnofsky or Eastern Cooperative Oncology Group scales for older patients before deciding on chemotherapy
- Chemo regimens are often cisplatin-based which carry the side effects of nephrotoxicity, ototoxicity, and neuropathy

Source: Nature Outlook
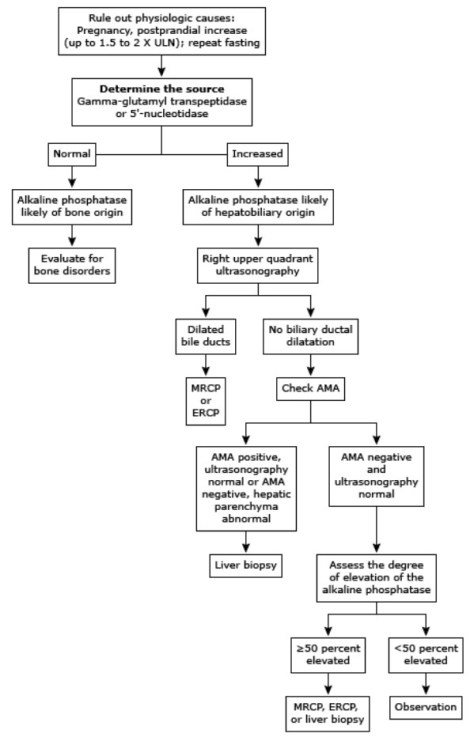
Hematuria
Refer to this thorough algorithm on UpToDate.
- Incidence of malignancy in microscopic hematuria is ~2-5%
- Incidence of malignancy in macroscopic hematuria is ~20%
Extra pearls on onset of hematuria during voiding:
- Occurs at the beginning? Urethral source
- Discharge noted between voidings or stain on undergarment? Urethral meatus or anterior urethra
- Terminal hematuria? Bladder neck or prostatic urethra
- Throughout voiding? Anywhere in the GU tract