Thanks to Sahar for presenting the interesting case of a middle-aged woman with metastatic melanoma recently started on ipilimumab who presented with a headache and fatigue, found to have hypothyroidism and adrenal insufficiency with work up consistent with hypopituitarism related to an adverse effect of ipilimumab: lymphocytic hypophysitis!
Clinical Pearls
- Remember that adrenal insufficiency and hypothyroidism are causes of elevated ADH levels.
- Red flags for obtaining head imaging for headache include age >55, sudden onset, positional, onset after trauma or exercise, fever, focal neuro findings, and immunosuppression.
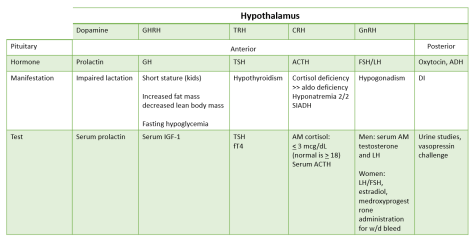
- Pituitary adenomas can have three manifestations: mass effect, hormonal hypersecretion, and hypopituitarism. When imaging shows a pituitary mass, your work up should address each of these categories.
- The most sensitive test to assess hypothalamic-pituitary access function is LH/FSH!
- Immunotherapies are commonly associated with a flare of autoimmune diseases. A more rare side effect of CTLA-4 inhibitors (like ipilimumab) is lymphocytic hypophysitis (inflammation of the pituitary gland)
- This condition commonly presents with headache out of proportion to neurologic findings and preferential decline in ACTH and TSH though other hormones can also be impacted.
- For hypopituitarism, remember to always treat adrenal insufficiency first before replacing thyroid hormone. Failure to do so can precipitate adrenal crisis!
Indications for imaging a patient with headache:
- Age >55
- Sudden onset
- Worse with lying down or wakes patient from sleep
- Rapid onset after trauma or exercise
- Fever
- Focal neurologic findings
- New headache in immunosuppressed patient
Pituitary adenoma:
- Evaluate for the following
- Mass effect: visual field deficit, headache
- Hormonal hypersecretion
- Prolactin ⇒ galactorrhea, amenorrhea, infertility
- GH ⇒ Acromegaly
- TSH ⇒ hyperthyroidism
- ACTH ⇒ Cushing disease
- ADH ⇒ SIADH
- Hyposecretion:
Hypophysitis:
- Inflammation of the pituitary
- Four categories based on histologic findings:
- Lymphocytic
- Most common form
- Seen in late pregnancy and post-partum period
- Also associated with ipilimumab as our patient here!
- Granulomatous
- Idiopathic or secondary to GPA, sarcoid, TB
- Plasmacytic (IgG4-related)
- Xanthomatous (most rare)
- Lymphocytic
- Clinical presentation
- Headache out of proportion to exam findings
- Preferential decrease in ACTH and TSH ⇒ adrenal insufficiency and hypothyroidism
- Prognosis:
- Pituitary size eventually normalizes but pituitary loss of function is often permanent.
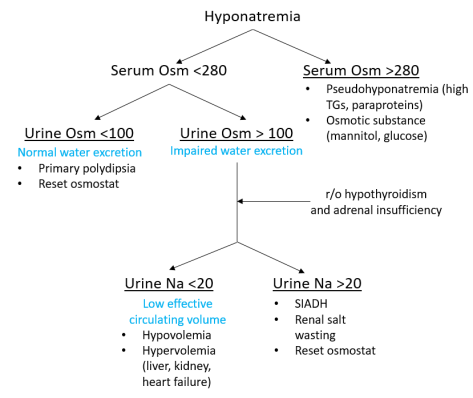
Hyponatremia:
Lastly, refer to this algorithm from our recent morning report to help you think through hyponatremia.
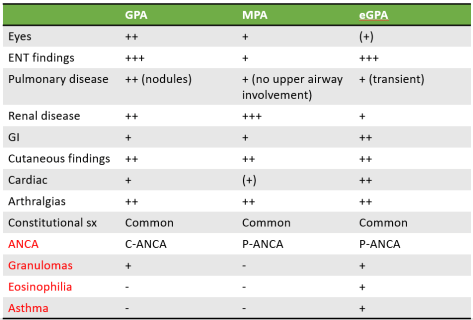




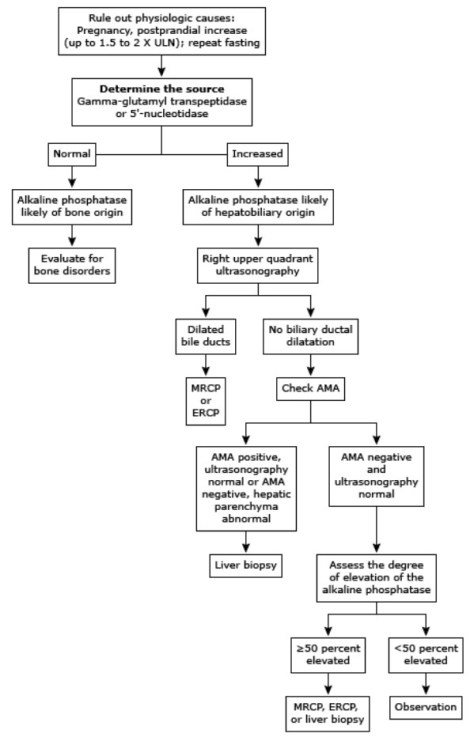
 Image adapted from Derm 101
Image adapted from Derm 101